

On CT chest, many pathologies can present with the same radiological findings. Hence a systematic approach is required to narrow down the differential diagnosis, and make appropriate recommendations. Dr Jankharia used various cases to discuss the approach to chest imaging. Here are few representative examples.
1. Approach to solitary pulmonary nodule
Solitary pulmonary nodule (SPN) is defined as a relatively well defined round or oval pulmonary parenchymal lesion equal or smaller than 30 mm in diameter. It is surrounded by pulmonary parenchyma and/or visceral pleura and is not associated with lymphadenopathy, atelectasis, or pneumonia.
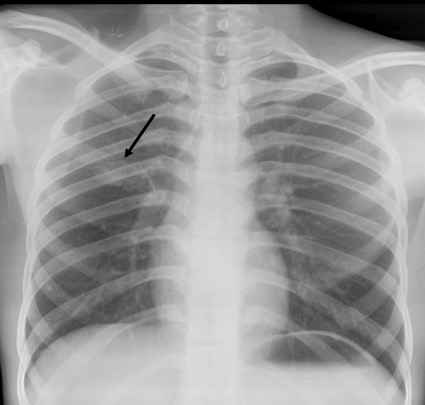
Frontal radiograph of the right hemithorax shows a relatively well defined approximately 2 cm sized oval soft tissue density nodule in the right middle zone. No calcification or cavitation. There is no other nodule. No effusion. No suspicious bone lesion.
Case courtesy of Dr Ayush Goel, <a href=”https://radiopaedia.org/”>Radiopaedia.org</a>. From the case <a href=”https://radiopaedia.org/cases/29150″>rID: 29150</a>
Note that the description of the nodule should always include its shape (round/oval, spiculated, lobulated etc), and presence or absence of cavitation and calcification. Unless the nodule demonstrates certain findings consistent with a benign etiology, it should be labelled as indeterminate and should be further evaluated with a CT/biopsy.

Criteria for benignity
- Presence of calcification (especially if is diffuse, popcorn, laminar, or central; eccentric or stippled patterns remain indeterminate)
- No contrast enhancement or uptake in PETCT
- No growth in 2 years (previous radiographs are hence considered to be equivalent to gold)
Doubling time rule
- Doubling in < 30 days: favors infection; it can also occur in aggressive hemorrhagic metastases like choriocarcinoma or RCC.
- Doubling in 30 to 465 days: favors neoplasm.
- Stability beyond this time period favors a benign etiology (there are rare exceptions like bronchoalveolar carcinoma, now reclassified as adenocarcinoma, with various subtypes).
Fleischner criteria
The Fleischner Society gave its recommendations for the follow-up of incidental pulmonary nodules detected on imaging in patients >35 years old. These do not apply to patients with a history of cancer or immunosuppression (as the nodule is not necessarily ‘incidental’ in these cases). The recommendations are based on the nodule density (solid vs subsolid), number (single vs multiple), size, and the patient’s cancer risk (history of smoking etc). A brief version of the guidelines can be found here, while the detailed Radiology 2017 guidelines article with numerous representative images and excellent review of literature is available here (highly recommended).
Given the absence of features of benignity on CT in our case, the impression on the CT would read:
Given the lack of any definite features of benignity, the nodule is indeterminate and a CT guided biopsy is recommended to differentiate between infection and neoplasm. (This particular case is an infection).
2. Lung cancer screening
Low dose non-contrast CT scan is used for screening of patients with history of smoking of at least 20 pack years (1 pack of 20 cigarettes/day for 20 years) between 50–79 years of age.
Lung CT Screening Reporting & Data System (Lung RADS)
Lung-RADS is a tool designed to standardize lung cancer screening CT reporting, ensuring uniform follow-up and management recommendations (similar to other such systems like BIRADS). Pulmonary findings are assigned risk categories from 1-4. It is different from the Fleischner criteria as it can be used only for CT lung cancer screening patients.
3. A 65-year old woman presented with history of acute breathlessness

CT pulmonary angiography shows significant partial filling defects involving the right and left pulmonary artery with extension to its lobar branches. Main pulmonary artery to aorta ratio is increased (greater than 1).
Case courtesy of Dr Jeremy Jones, <ahref=”https://radiopaedia.org/”>Radiopaedia.org</a>. From the case <a href=”https://radiopaedia.org/cases/13211″>rID: 13211</a>
The other imaging findings to be mentioned (as they indicate prognosis) are:
- Thrombus burden (subjective)
- Right ventricle: Left ventricle ratio (normal<0.9)
- Changes in bilateral lungs (infarcts)
- Contrast reflux into IVC (due to high pressure in the right atrium).
The most important poor prognostic indicator is increased RV/LV ratio which is a sign RV strain.
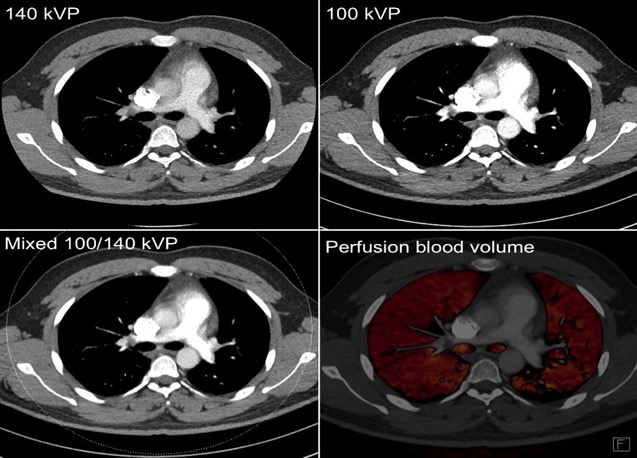
Case courtesy of Dr Charlie Chia-Tsong Hsu <ahref=”https://radiopaedia.org/”>Radiopaedia.org</a>. From the case <a href=”https://radiopaedia.org/cases/31363″>rID: 31363</a>
Dual energy perfusion maps can be used for quantitative assessment of the effects of PTE. They may also be used for follow up, post anticoagulation treatment.
4. Mediastinal lymphadenopathy

Contrast enhanced CT scan of thorax, showing multiple relatively symmetric well defined mildly enlarged non-necrotic nodes in the paratracheal and aortopulmonary regions.
The common differential diagnosis includes:
a. Tuberculosis: The presence of necrosis within the node favors TB as the diagnosis. However TB can also present with non-necrotic nodes; so the absence of necrosis is not as useful a feature.
b. Sarcoidosis: It usually presents as bilateral symmetric hilar, paratracheal, and subcarinal adenopathy, without bulky prevascular nodes. Lung nodules in perihilar, perilymphatic, and perifissural distribution are diagnostic.


c. Lymphoma: It usually presents with enlarged confluent prevascular adenopathy.

Case courtesy of A.Prof Frank Gaillard, <ahref=”https://radiopaedia.org/”>Radiopaedia.org</a>. From the case <a href=”https://radiopaedia.org/cases/8655″>rID: 8655</a>
d. Metastasis: Metastasis is a great mimicker, and should always be a differential in older patients.
5. Incidental finding in a 30 year old man who has undergone health check up.

Scout CT topogram shows an elongated soft tissue opacity in the right paratracheal region in the superior mediastinum, with a well-defined superior margin extending above the clavicle. This is hence a posterior mediastinal mass (cervicothoracic sign).
Cervicothoracic sign: At the level of the thoracic inlet, the posterior part of the lung extends superior to the clavicle compared to the anterior part; hence, any mass when situated in the posterior mediastinum, is completely surrounded by lung tissue from all sides. This leads to a well-defined cephalic border seen above the clavicle. In contrast to this, anterior mediastinal masses have ill-defined cephalic margins due to their anatomical contact with the soft tissues of the neck.
In summary,
1. Whenever you encounter a solitary pulmonary nodule, evaluate it objectively. If there are no features of benignity, recommend follow-up (Fleischner criteria), CT or biopsy depending on the clinical scenario. Always ask for prior imaging if available.
2. Lung cancer screening is possible in select people with history of smoking over 20 pack years.
3. Look for signs of right ventricular dysfunction when reporting pulmonary thromboembolism.
4. The differentials for mediastinal adenopathy are limited and age-based, and should be worked up appropriately.
5. Know the classic radiology signs such as the cervicothoracic sign!
– Anjitha Subhash, Tata Memorial Hospital

do this have video lectures
LikeLike
Yes they do. We have four free to attend webinars every week (we have completed over 550 webinars). You can see the list of upcoming webinars on this website at https://caferoentgen.com/wednesday-webinar/. You can also see the webinar recordings at https://www.themeditube.com/best_deals/751
LikeLike