

Dr Meher Ursekar took a brilliant lecture on neuroanatomy last month, correlating brain anatomy, function, and functional MRI. It took some time to prepare notes because of the relatively abstract nature of the topic; besides it was difficult to obtain figures for each and every structure we are talking about. Apologies for the delay. We would suggest googling whenever you have a doubt about the anatomy to look at relevant images. There are a few helpful links at the end which should also be kept open in the next tab while going through the notes.
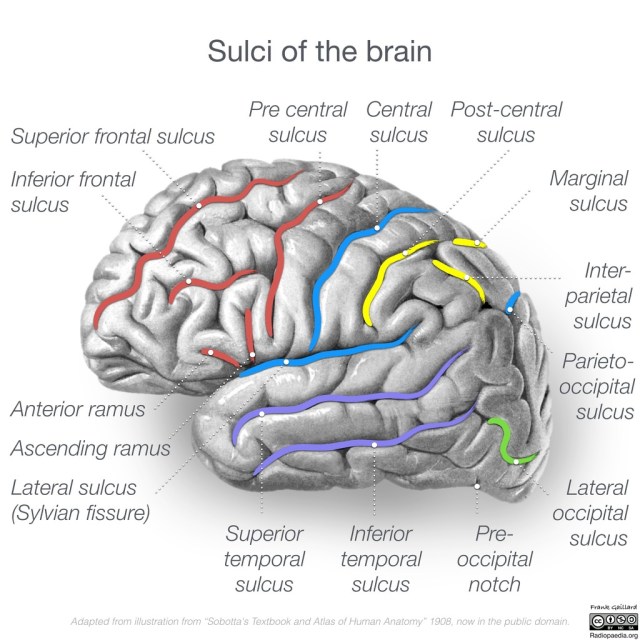
1. Fissures are really deep sulci. There are overall 14 major sulci:
Major Sulci (14):
Typically continuous sulci (6):
- Interhemispheric fissure
- Sylvian fissure
- Parieto-occipital fissure
- Collateral sulcus
- Central sulcus
- Calcarine sulcus
Typically discontinuous sulci (8):
- Precentral sulcus
- Superior frontal sulcus
- Inferior frontal sulcus
- Postcentral sulcus
- Intraparietal sulcus
- Superior temporal sulcus
- Inferior temporal sulcus
- Cingulate sulcus
Case courtesy of A.Prof Frank Gaillard, <ahref=”https://radiopaedia.org/”>Radiopaedia.org</a>. From the case <a href=”https://radiopaedia.org/cases/46670″>rID: 46670</a>
2. Interhemispheric fissure
It divides the brain into two lobes, which are functionally asymmetric but anatomically symmetric
Left lobe: is dominant and controls speech, amongst other things
Right lobe: is non-dominant, and controls spatial relationships (recognizing patterns, forms) and musical expressions, amongst other things.
The bridge between the hemispheres is the corpus callosum and the anterior commissure.
3. Sylvian fissure
It forms an M shaped inferior frontal gyrus anteriorly (containing Broca’s area), while posteriorly it forms a fish tail and mounts the supramarginal gyrus superiorly.
In the middle of the sylvian fissure, there is a ‘smiling’ portion- the pre and post central gyrus meet here to form subcentral gyrus (has motor control of tongue, lip, and larynx).
Minor rami arising from Sylvian fissure: anterior subcentral, posterior subcentral
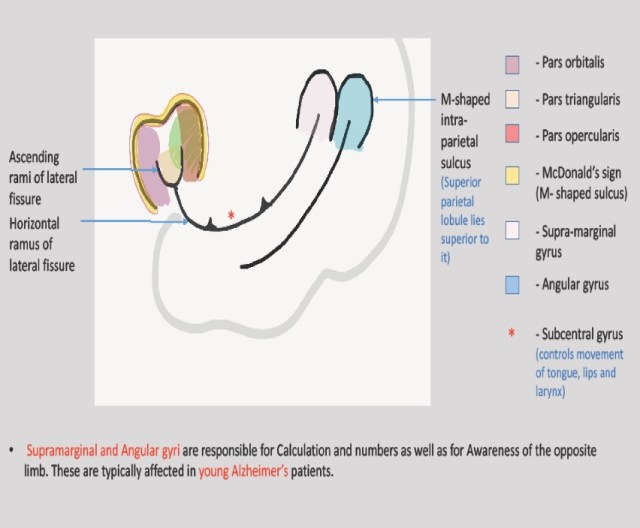
– Artwork by Dr Neeti Gupta, Radiology Resident, Tata Memorial Hospital
4. Superior and inferior frontal sulci
The superior frontal sulcus separates the superior frontal gyrus and the middle frontal gyrus. On the other hand, the inferior frontal sulcus separates the superior frontal gyrus and the inferior frontal gyrus.
The superior frontal sulcus curves upwards and forms part of precentral sulcus, while the inferior frontal sulcus curves downwards and forms part of precentral sulcus.
Hence, precentral sulcus is discontinuous; this is the portion where middle frontal gyrus and the precentral gyrus are continuous.

Case courtesy of A.Prof Frank Gaillard, <ahref=”https://radiopaedia.org/”>Radiopaedia.org</a>. From the case <a href=”https://radiopaedia.org/cases/33834″>rID: 33834</a>
5. Frontal lobe: It has-
Superior frontal gyrus- is loooooong!
Middle frontal gyrus- is zigzag
Inferior frontal gyrus- forms an M (looks like the McDonalds ‘M’)
Precentral gyrus- is vertical

Case courtesy of A.Prof Frank Gaillard, <ahref=”https://radiopaedia.org/”>Radiopaedia.org</a>. From the case <a href=”https://radiopaedia.org/cases/33834″>rID: 33834</a>
6. Insula/ Island of Reil (island of grey matter)
The insular cortex consists of a large anterior insula and a small posterior insula. The cortical area overlying the insula towards the lateral brain surface is called the operculum.
Anterior and posterior insula are separated by central insular sulcus Note that the central and precentral sulcus cut through the insula.
Anterior insula- motor tasks, amygdala activation, social emotions, language, motor tasks, amygdala, interceptive awareness: cortex thickened by meditation. Seen in resting state, fMRI studies.
Posterior insula- time or decision making, audition or speech
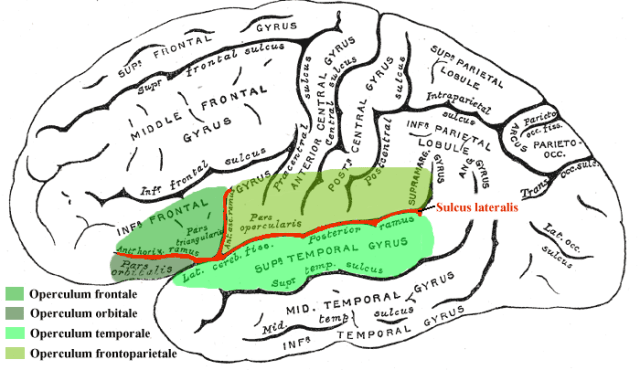
Image by User: Uwe Gille (Gray’s Anatomy FIG. 726, modified by me) [Public domain, Public domain or Public domain], via Wikimedia Commons
7. On an axial section:
Superior frontal sulcus: trace back to precentral sulcus (is perpendicular to it). The frontal eye field is located at junction of the two.
The sulcus behind this is the central sulcus. This may help identify the central sulcus in uncertain cases.
8. Motor function: There are three components to motor function.
Imagining- prefrontal
Planning- premotor cortex
Execution- motor cortex
Thus, for finger tapping assessment on fMRI, the order of activation would be
Imagining: Proprioception (where are my fingers) – joint → thalamus → post central gyrus (primary central cortex) → post parietal cortex
Planning: premotor cortex, supplementary motor area
Execution: primary motor cortex
Any abnormality in this pathway can impact the fMRI findings.
9. There are six major motor areas:
- Primary motor cortex
- Supplementary motor cortex
- Premotor
- Pre-supplementary
- Cingulate
- Prefrontal
Most of these can be identified anatomically. However, a functional study is useful when sulcal anatomy is blunted or effaced (as in tumors etc).
Cerebellum is a fantastic way of localizing supplementary motor area (it crosses to opposite in cerebellum)
Damage to the supplementary motor area causes motor akinesia, one can’t plan movement. But since this area is bilaterally represented, patients can recover function in time.
10. Language
Hearing → primary auditory cortex→ Wernicke’s→ Broca’s→ motor cortex
Sylvian fissure is closely related to the auditory cortex.
Supramarginal and angular gyrus: take care of the nuances of language
Broca’s and Wernicke’s: are connected by the arcuate fasciculus
To activate Wernicke’s area on fMRI:
In adults- category repetition task- show apple-is it fruit etc
In children- tell a story and ask to repeat
To activate Broca’s (posterior part of McDonald’s M) on fMRI: word generation, verb generation, noun-verb relation task (generate verb from noun)
When left handed: 70% are left dominant
30% are right dominant/bilateral
Tumor in superior temporal gyrus may affect auditory function and Wernicke’s area.
11. Watershed zones are
- Superior frontal sulcus- ACA and MCA
- Intraparietal sulcus- MCA and PCA
12. Heschl’s gyrus:
This is a bump on the superior temporal gyrus/posterior part of sylvian fissure. This is an auditory area, and is not a part of insula. It has an elongated appearance. It is stimulated by pure tones.
Tonotopia is a way of mapping each pitch on the temporal lobe, to map the auditory cortex. We do this when planning for cochlear implant. You must give auditory stimuli in the silent portion of the RF beat; it is visualized towards the lag end of the hemodynamic response.
13. Cuneus: medial surface of occipital lobe above calcarine fissure, contains V1,2,3
Lingual part of occipital lobe: face and object recognition

Case courtesy of A.Prof Frank Gaillard, <ahref=”https://radiopaedia.org/”>Radiopaedia.org</a>. From the case <a href=”https://radiopaedia.org/cases/47208″>rID: 47208</a>
14. Along the medial surface, the cingulate sulcus turns upwards (pars marginalis) and separates the frontal and parietal lobes. It lies just posterior to the central sulcus on axial section – the bracket sign (the bracket is formed by the pars marginalis bilaterally on axial images, anterior to it is the central sulcus foot and bladder area). On the medial surface as well, the central sulcus is anterior to the pars marginalis and perpendicular to it. At its inferior end is the paracentral lobule.
15. With reference to understanding an fMRI activation: Please note that the motor area is the adjacent bank of grey matter just adjacent to the central sulcus anteriorly (similarly for sensory cortex posteriorly). However, we see activation of the precentral gyrus because that’s the vascular zone which will be depicted on BOLD imaging (similarly for sensory cortex posteriorly).
More information:
i. There is a nice ppt on this topic at https://www.google.co.in/url?sa=t&source=web&rct=j&url=http://ece-research.unm.edu/vcalhoun/courses/fMRI_Spring07/Lecture03_BrainAnatomy.pdf&ved=0ahUKEwi16LfCmKLYAhXKNY8KHazWA6UQFggnMAE&usg=AOvVaw35bUkftA3NMYfoMxsDrbjY
ii. There are some nice neuroanatomy diagrams on the following link: http://www.cengage.com/resource_uploads/downloads/084003265X_249272.pdf
– Nikshita Jain, Senior registrar, Tata Memorial Hospital
– Akshay Baheti, Assistant Professor, Tata Memorial Hospital
