

Sachin is Assistant Professor in Pediatric Radiology at Medical College of Wisconsin. He conducted a fantastic session on pediatric foot alignment (and on pediatric elbow injuries: see the previous blog). Many of the images in this blog and the previous one are also contributed by him; a huge thanks!
There are a lot of technical terms and angles and lines introduced in the blog. If they become too much, just understand three lines at the minimum: midtalar line, midcalcaneal line, and talocalcaneal angle, and then go to the steps to be followed while reporting a foot alignment radiograph.
Introduction
The basic radiographic examinations required for assessment of any foot deformity are anteroposterior (dorsoplantar) view and lateral view.
Each radiograph must be taken in weight bearing position. Non weightbearing radiographs are inadequate as they do not show bones in their functional states. You cannot comment on foot alignment in a non weight bearing radiograph. Simulated weight bearing radiographs are taken in infants and non-ambulatory patients by applying plantar pressure with a plastic board.
The AP projection is taken in the standing position with tibia perpendicular to the film plane and x-rays directed 150 posteriorly. The tibia should be perpendicular to the cassette even on a lateral film.
Nomenclature
A. Division of foot:
- Hindfoot: consists of talus and calcaneum.
- Midfoot: rest of the talar bones.
- Forefoot: metatarsal and phalanges.

B. Lines and angles:
- Midtalar line: passes along the long axis of talus, parallel to its medial cortical surface. It should pass through or immediately medial to the base of 1st metatarsal on AP and lateral view (note that the relation is with the base, and not the shaft, of the metatarsal).
- Midcalcaneal line: passes along the long axis of calcaneum, parallel to its lateral cortical surface. It should pass through or close to the base of 4th metatarsal on AP view.
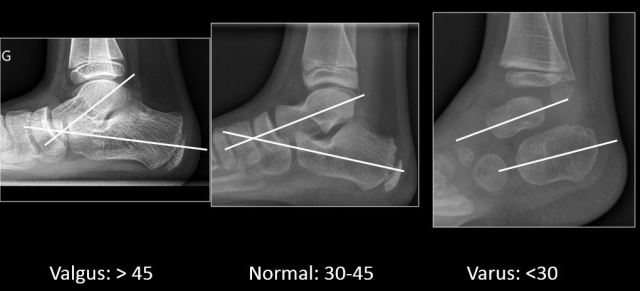
- Talocalcaneal angle: the angle formed between midtalar and midcalcaneal line. Normal: 300-450; <300: varus; >450: valgus.
- Tibiocalcaneal angle: angle formed between the long axis of tibia and mid calcaneal line on lateral radiograph. Normal: 700-900; >900: equinus; <700: calcaneus.
‘a’, ‘b’ and ‘c’ are valid for both AP and lateral radiographs while ‘d’ can be calculated only on lateral radiographs.


Midtalar line, midcalcaneal line, and talocalcaneal angle on AP and lateral views

Tibiocalcaneal angle
C. Types of deformity:
I. Abnormalities in foot alignment:
- Valgus: increase in talocalcaneal angle (>450) with midcalcaneal line deviated away from midline.
- Varus: decrease in talocalcaneal angle (<300) with midcalcaneal line deviated towards midline (r in the va’r’us is for ‘reduction’ of angle).
- Equinus: posterior end of foot elevated superiorly.
- Calcaneus: anterior end of foot elevated superiorly.
- Cavus: increase in the depth of longitudinal arch (formed by metatarsals and calcaneus).
Valgus and varus are best evaluated on AP view while equinus, calcaneus and cavus are best evaluated on lateral view.
II. Abnormalities of forefoot (Movement strictly in the plane of foot with no element of rotation. Best evaluated on AP view)
- Adduction: movement of forefoot towards midline with respect to mid and hindfoot.
- Abduction: movement of forefoot away from the midline.
- Inversion: varus + supination.
- Eversion: valgus + pronation.
STEPS TO BE FOLLOWED WHILE REPORTING A FOOT ALIGNMENT RADIOGRAPH
AP radiograph
- Remember that the talus is considered to be the centre of the foot and any movement of any bone is described with respect to talus. This is because the talus is the only foot bone without any direct muscular attachment (it is held in place by ligaments alone) and majority of diseases causing foot malalignment are either neurological or neuromuscular and would lead to altered positions of the attached bones accordingly.
- Confirm that the x-ray is taken in weight-bearing position.
- Identify talus and calcaneum. Talus is the medial bone and calcaneum the lateral. Anterior of talus is convex and more anterior than the anterior end of calcaneum which is flat in adults, but can be convex in children. (This may sound silly but is not always easy in a small child when all we see are a few tiny ossification centres).
- Evaluate the talocalcaneal alignment by drawing midtalar and midcalcaneal line and calculating talocalcaneal angle.
- Evaluate the talonavicular alignment (alignment between hindfoot and midfoot). Normally the navicular bone is positioned directly opposite the talus throughout its extent.
- Check for the overlap of the metatarsal bases to rule out inversion and eversion. Normally, there is slight amount of overlap.
Lateral radiograph (upright radiograph is essential)
Steps are basically same as that on AP radiograph with modifications enlisted.
- Normally, long axis of talus is directed anteroinferiorly, while that of calcaneum anterosuperiorly. When the calcaneum moves towards the talus i.e. varus, it lifts up the talus and it is vice versa in valgus deformity. Usually the varus deformity is associated with cavus (cavovarus) and planus deformity with valgus.
- There is substantial overlap between the metatarsals, even more than that on AP view, with the 5th metatarsal being the inferiormost.
- Apart from calculating the talocalcaneal angle, also calculate the tibiocalcaneal angle.
Two additonal points to be noted on the lateral radiograph:
- Look for calcaneonavicular or calcaneotalar coalition. It is an easily correctable deformity and hence important to catch and report.
- Dorsal edges of talus and navicular bone are at the same horizontal level, called talonavicular association. When they are at different level, it is called talonavicular dissociation. In a case of valgus deformity, look for talonavicular association. If it is maintained, it is flat foot. If it is disturbed, then the diagnosis is congenital vertical talus (rockerbottom foot).
CASES:
1.


On AP, the midtalar line passes lateral to the base of 1st metatarsal which is abnormal. The midcalcaneal line is passing through the base of 4th metatarsal which is normal. Thus the alignment is abnormal. The talocalcaneal angle is reduced (<30 degrees).
On lateral as well, the talocalcaneal angle is reduced, and the talus appears lifted up by the calcaneus. This is thus a hindfoot varus deformity.
2.


Image by Michael Nebel http://de.wikipedia.org/wiki/Benutzer:Jakker [CC BY-SA 2.0 de (https://creativecommons.org/licenses/by-sa/2.0/de/deed.en)%5D, via Wikimedia Commons
On AP, the midtalar line passes much medial to the base of 1st metatarsal than expected, which is abnormal. The midcalcaneal line is passing through the base of 4th metatarsal which is normal. Thus the alignment is abnormal. The talocalcaneal angle is increased(>45 degrees). On lateral as well, the talocalcaneal angle is increased. This is thus a hindfoot valgus deformity.
In conclusion,

This is not supposed to be an exhaustive review; to see some great cases as also reinforce your concepts, please look at the article link below.
https://www.ajronline.org/doi/full/10.2214/AJR.07.7143
– Shehbaz Ansari, Radiology resident, Seth GSMC & KEMH.
– Akshay Baheti, Assistant Professor, Tata Memorial Hospital

Ultimate class and notes..
LikeLike