

Sumeet is Assistant Professor in Neuroradiology at Rush University, Chicago. He showed very interesting cases as examples to demonstrate various vascular pathologies. All the images in this blog and the subsequent one are also contributed by him; a huge thanks!
Case no.1: Intracranial atherosclerotic disease – 54 yr old male, presenting with R sided weakness, prior strokes, k/c/o HTN, DM.
Small lacunar infarcts occur due to small vessel disease, wedge shaped peripheral infarcts are usually due to embolism, watershed infarcts occur due to global hypotension and associated carotid plaques, and large arterial territory infarcts are seen in complete vessel occlusion.
Apart from routine MRA, Vessel Wall Imaging (VWI) may be performed in cases where there are other differentials (discussed below); culprit atherosclerotic plaques may demonstrate eccentric enhancement.

High resolution vessel wall imaging (A & B) shows eccentric enhancement involving the inferior wall of the cavernous left internal carotid artery and minimal concentric enhancement on the right.
Case no. 2: Moyamoya disease

Coronal MIP CT angiogram (A) and right carotid injection DSA (B) showing bilateral severe ICA & MCA narrowing with puff of smoke appearance. Oblique MIP CT angiogram of the neck showing champagne-bottle neck sign seen in advanced cases of Moyamoya disease.
The classic puff-of-smoke appearance of lenticulostriate & thalamostriate collaterals is seen on DSA. Equivalent collateral vessels may be seen on CTA/MRI.
Presence of Champagne bottle neck sign of ICA in the neck suggests a more severe disease and worse prognosis. Please read the AJNR article below for more details.
http://www.ajnr.org/content/37/10/1898
Case no. 3: Arterial dissection – c/o vertigo with history of minor neck manipulation
B/L cerebellar hemispheres infarcts (images not shown) due to arterial dissection seen in the case.

Coronal post contrast MRA (A) shows tapered narrowing and occlusion of the right vertebral artery. Axial T2 weighted (B) and axial black blood T1 weighted (C) images show absence of flow void and T1 hyperintensity in the right V2 segment respectively.
Most common presenting complaint is neck pain. CTA/ MRA may detect it. Black blood sequence will demonstrate an eccentric intramural T1 hyperintensity, which represents subacute dissected blood.
Importantly, as the patient may complain of neck pain and not focal neurological deficit; the first investigation performed may be an MRI of the cervical spine! Hence, always look at the vertebral artery flow void in all cervical spine patients.
Case no. 4: CNS Vasculitis – 54yr/F, presents with headache and focal deficit.
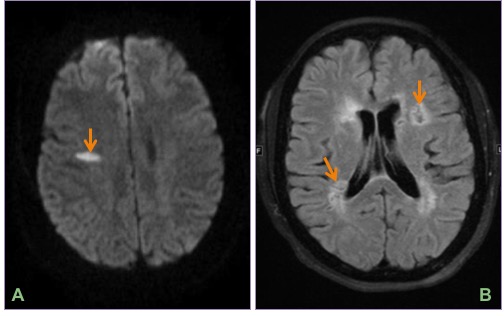
Axial DWI (A) and FLAIR (B) images show an acute infarct in the right centrum semiovale and multiple remote infarcts in bilateral periventricular white matter.
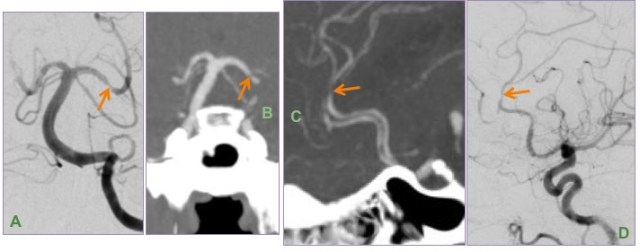
DSA (A & D) and MIP images from CTA brain (B & C) show multifocal short segment stenosis of medium-sized intracranial arteries of the anterior and posterior circulation.
Leptomeningeal biopsy showed vasculocentric transmural inflammation of the small arterioles with fibrinoid necrosis, consistent with vasculitis.
Vessel wall imaging may be performed in this case to look for homogeneous circumferential wall enhancement.
Note that CNS vasculitis may present with headache as well rather than focal neurological deficit.
Case no. 5: Reversible cerebral vasoconstriction syndrome (RCVS). 22/F, thunderclap headache, on SSRI’s.

Axial FLAIR image (A) and minimum intensity projection (minIP) SWI image (B) showing minimal acute high parietal convexal subarachnoid hemorrhage.

MIP-MRA (A) showing diffuse beading of the A1 & M1 segments & distal branches. Based on the clinical presentation and imaging findings, a diagnosis of reversible cerebral vasoconstriction syndrome (RCVS) was suggested.
RCVS occurs in patients on vasoactive drugs such as SSRIs, with thunderclap headache due to SAH being the classic history.
Reversible vasospasm is essential for diagnosis; irreversibility suggest vasculitis. Follow-up DSA/MRA can be performed to demonstrate reversibility. On vessel wall imaging, RCVS will not enhance as opposed to vasculitis, and this can be performed to differentiate between the two if there is a doubt.
PRESS is probably a continuum of RCVS.
On the topic of FLAIR sulcal hyperintensity, a good article to read on the differentials is on the link below.
https://www.ajronline.org/doi/full/10.2214/AJR.07.2424
RCVS vs CNS Vasculitis
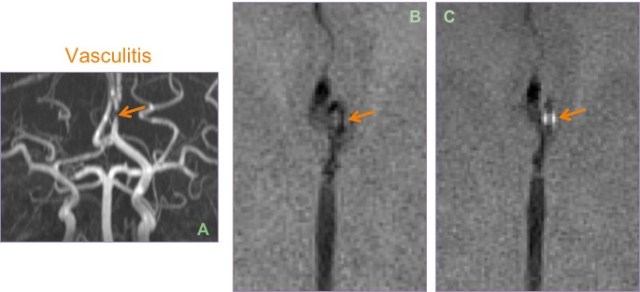
Biopsy proven case of CNS vasculitis. Severe focal stenosis of the left A2 segment noted on the MIP-MRA (A); enhancement of the stenosed sesgment is seen after contrast administration on post VW image (C). Pre (B) image is shown for comparison.
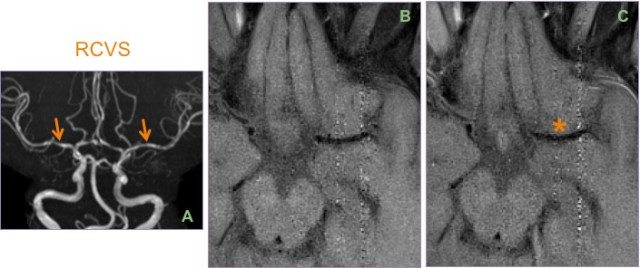
Contrast this case of RCVS (A), where there is no abnormal enhancement * of the wall of the vasoconstricted M1 segment between the pre (B) and post (C) VW images.
Case no. 6: Cocaine-induced vasculopathy – 26/F, acute vertigo with vision loss, toxic screen positive for cocaine.
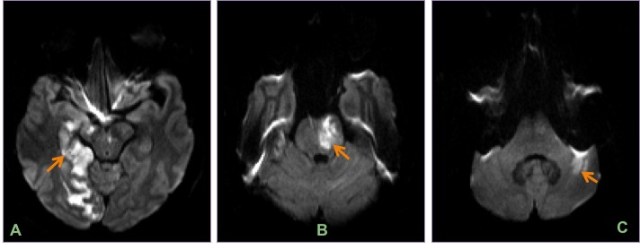
Axial DWI images show multiple acute posterior circulation infarcts involving the right occipital lobe (A), brainstem (B) and left cerebellar hemisphere (C).

Oblique coronal MIP CT angiogram reconstructions (A & B) and left vertebral injection DSA (C) from the same patient show diffuse beading of the vertebral & basilar arteries.
Cocaine-induced vasculopathy can cause ischemia or can cause subarachnoid or intra-parenchymal bleed, with the distribution of bleed being same as that of hypertensive one. Diffuse beading of vessels is seen on DSA.
Case no. 7: SAH – 32/F with SAH due to PCA aneurysm, Modified Fisher grade 4
Modified Fisher scale must be given while reporting any SAH due to aneurysmal bleed, as the incidence of reactive vasospasm increase with worsening grade. Note than thin SAH refers to <1 mm depth, while thick SAH refers to ≥ 1 mm depth.
Grade 1: Focal or diffuse thin SAH without intraventricular hemorrhage (IVH)
Grade 2: Focal or diffuse thin SAH with IVH
Grade 3: Focal or diffuse thick SAH without IVH
Grade 4: Focal or diffuse thick SAH with IVH
The incidence of vasospasm increases from 6-24% in grade 1 to 40% in grade 4 SAH.
Vasospasm (also called as delayed cerebral ischemia) can be in SAH, probably due to irritation by the subarachnoid blood products. It peaks on day 4-8, and shows narrowing and irregularity of arteries in the circle of Willis on DSA/MRA. Trans-cranial Doppler (TCD) studies may be used for monitoring in patients with SAH.
Case no. 8: Meningitis – c/o altered mental status, fever.
Vasospasm can be seen in meningitis due to associated vasculitis, reversible spasm or intimal proliferation. TCD may be used for monitoring. Lindegaard ratio (MCA velocity/extracranial ICA velocity) > 3 on TCD indicates presence of vasospasm on TCD.
Case no. 9: Vasospasm in operated skull based tumors – operated c/o CP angle schwannoma on day 4 post-op, develops lethargy and speech difficulty, due to infarct.

Axial T2 weighted image (A) through the posterior fossa shows a CPA schwannoma. DWI image (B) shows a wedge shaped right parietal acute infarct and smaller acute infarct in the left centrum semiovale, both in watershed zones.

MIP image from MR angiogram (A) shows beaded narrowing of the right M1 segment. DSA images (B & C) confirm the finding seen on the MRA with narrowing of bilateral M1 segments, more pronounced on the right side (side of the infarct).
The etiology of this entity is unknown as the vasospasm and infarct can occur even in say the anterior circulation vessels despite it being a posterior fossa surgery (it is not related to direct surgical handling or trauma). It is more commonly seen after skull base surgeries in the posterior fossa. Vessel irregularities are seen on MRA/DSA.
Thus, many of these etiologies may appear similar on MRA/DSA, with vessel irregularity, narrowing or beading. However, the appropriate clinical context with or without vessel wall imaging can help narrow the differentials.
Articles for further reading on vessel wall imaging:
http://www.ajnr.org/content/ajnr/early/2016/07/28/ajnr.A4893.full.pdf
https://nvijournal.biomedcentral.com/articles/10.1186/s40809-016-0014-5
– Aneree Shah, DNB Radiology, Jupiter Hospital, Thane
– Akshay Baheti, Assistant Professor, Tata Memorial Hospital
– All images and legends courtesy Sumeet Dua, Assistant Professor, Rush University, Chicago

What about fibromuscular dysplasia as a ddx for beading? Thanks for sharing!
LikeLike