

Duration: Three years
Number of seats: Entrance exam is held twice yearly for July and January sessions. The number of seats is as follows.

N.B: Sponsored seat = service category seat (eg armed forces/ govt institute/ foreign national sponsored candidates). Deputation/Sponsorship of any candidate by private hospitals, institutes or nursing homes are not accepted. The service category seats are not transferred to general or open category and remains vacant if no eligible candidates are found, which was very frequent until 2018. At a particular time, there are about 10 DM residents.
Application forms for the entrance exam are usually available on the website pgimer.edu.in 3-4 months prior to the start of the session. Entrance exams are usually held a month before the start of the session. Results are declared within 5-7 days. Selected candidates get about 2-3 weeks to join the Institute after the results are declared. Entrance exam dates might change due to administrative or academic reasons, so it is advised to check the website regularly for latest notification/ announcement as well as any Addendum/Corrigendum/Latest updates regarding the Examination.
P.S Computer-based test was held for the July 2020 session in view of the COVID19 outbreak.
Accreditation: Like NIMHANS and AIIMS, PGIMER is an autonomous body and thus awards its own DM degree.
Entrance exam pattern: PGIMER has removed practical examination from the selection criteria. Thus, it is a single step theory only examination now, comprising of 80 multiple choice question (MCQs) with five alternatives each and single/multiple correct responses.
The theory examination consists of a paper with two parts (Part 1 – General Radiology, and Part 2 –Neuroradiology), each with 40 marks. Part 1 consists of 40 multiple choice questions, each with four options and a single most appropriate response. The questions will cover all the aspects of General Radiology (MD level) including few questions on statistics, radiation protection and radiophysics. Part 2 of the paper consists of 40 multiple choice questions related to the neuroradiology, each with five options and single/multiple correct response(s). The duration of examination is usually 90 minutes. Each question correctly answered in Part 1 is awarded one mark, with no negative marking for wrong answers. Incorrect responses are, however, negatively marked in Part 2 of the paper. This part has 40 questions, each with five response options. Hence there are a total of 200 response options. One or more of these five options can be correct for each question. True correct responses (i.e. candidate correctly marks a response as true) are marked positively, and incorrect responses (i.e. candidate marks an incorrect response as correct) are scored negatively. Any responses not marked by the candidate are not scored. A similar pattern was followed for the computer based exam held in June 2020.
Based on the theory score, a rank list is prepared and the candidates are called for counselling as per merit.
Expected marks for getting a seat: A score between 58-65 (out of 80) might possibly get you top rank in open category. But the cut-off varies year to year. A separate rank list is made for sponsored candidates.
Tips on how to secure the DM seat: There are no specific MCQ/ question banks to guide you for the DM entrance exam, especially for DM neuroradiology. MCQ’s in FRCR/ EDIR question banks can be tried to gain confidence. For general radiology (part 1), don’t forget to read about radiation protection and basic physics. Questions are straight forward and relatively easy to answer. For neuroradiology (part 2), you might be asked recent neuro intervention related questions especially on stroke, flow divertors, neuro intervention hardware etc. Two or three questions are usually from paediatric neuroradiology, demyelination and glioma genetics, and current classification.
Interventions and Hands-on experience: PGIMER has a common Department of Radiology. However, the neuroradiology roster is separate from general radiology senior residents. PGIMER has also introduced DM in Interventional Radiology form July 2020. Unlike other institutes like AIIMS or NIMHANS, the advantage of doing DM at PGIMER is that you will get hands-on experience in neuro as well as non-neuro vascular and non-vascular interventions (since we get one month of posting in general radiology every 6 months, interested candidates can ask for non neuro interventions or Body MRI or USG; anything they wish to learn). As of now, the dept has a total of 6 neuroradiology faculty members; most of them look after Neuro-intervention. The DM neuro roster is made once for every 6 months. The rotation is for 1 month in each modality. Usually 4 residents are posted in MRI (including paediatric and trauma centre MRI), 2 in DSA, 1 in CT, 1 in neuro-intervention OPD and 1 in night duty.
Modalities available in the Department: The Department has 5-6 CT scanners, 5 MRI scanners (including 1 standing open gantry MRI), 2 DSA machines (one Philips biplane for neuro interventions and one Philips single plane for body interventions). PET/SPECT are managed by Nuclear medicine department.
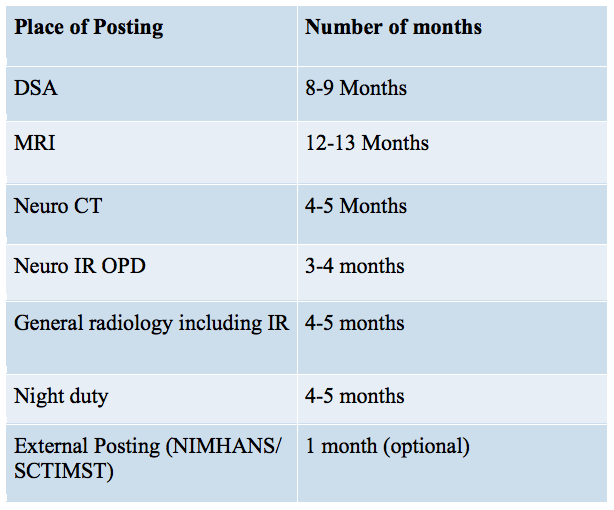
The entire 36 months of DM at PGIMER are divided approximately as following:
DSA workload: The division of Neuro intervention at PGIMER does not have patient admission rights. So the patients are admitted under neurology or neurosurgery and sent to us only for intervention. Though PGIMER get referrals from most of North India (4-5 states) and is one of Asia ‘s top institutes in terms of number of referrals for cerebral aneurysms, the case load for endovascular treatment is not very high when compared to clipping done by neurosurgeons. Post procedure patients are managed by the admitting physicians, though ward rounds are a must for neuro intervention residents.
Here is a rough estimate of the case load:
Diagnostic cerebral and spinal DSA cases (including intra-arterial Nimodipine) – approximately 100-120/ month.
Sclerotherapy for head and Neck low flow malformations: 100-120 / month.
Neuro-intervention cases: Varies on an alternate monthly basis (range: 15–30/ month);10-12 aneurysm coiling, 4-6 mechanical thrombectomies, 1-2 carotid stenting/ AVM embolisations/ spinal vascular malformations, 1-2 head-neck pseudoaneurysms, 2-3 pre-op tumour embolisation/ high flow head and neck AVM embolisations.
DSA posting starts from second semester. In the first month of DSA, you get to know about basic workflow, flow of finances, and departmental protocols. You get trained in doing diagnostic cerebral and spinal angiograms under the supervision of senior SR. You get to know basic neuro intervention hardware and vascular anatomy. At the same time, you get to assist the seniors and faculty in all major intervention cases. Usually by the end of second- third posting, you become confident to do all diagnostic DSAs and pre op tumor/head-neck AVM embolisation (if you are lucky and enthusiastic) on your own without requiring the supervision of senior SRs.
Most of the hands-on training in major neurointervention cases is given in the final semester. You do get hands-on in a limited number of cases; based on the complexity of the case and depending on the faculty who is doing the case. It remains the final decision of the faculty in–charge whether to allow you to put a coil in an aneurysm or inject Onyx or allow you to do a Mechanical thrombectomy. As far as I am concerned, I have done 3 mechanical thrombectomies (but under the supervision of the consultant in-charge), aneurysm coiling in 3 cases (FD deployment in one case under supervision), two Onyx injections (one in case of right temporal AVM supplied by MMA, other in case of right transverse sinus dAVF), 8-10 neck pseudoaneurysm embolisation, 6-8 pre-op tumor/ high flow AVM embolisations, 7-8 cases of IPSS, 2 cases of CCF and 2 carotid stentings. How much hands-on you will get varies and will depend on your luck, availability of junior faculty and the “season” of your DSA posting (definitely more emergency cases in winters).
Academic activities: All the journal clubs/ seminars/ presentations are done by SRs (on a six monthly roster basis) in PowerPoint format. The fifth semester SR’s represent us in the Neurology-neuroradiology rounds. The weekly academic roster is as follows:
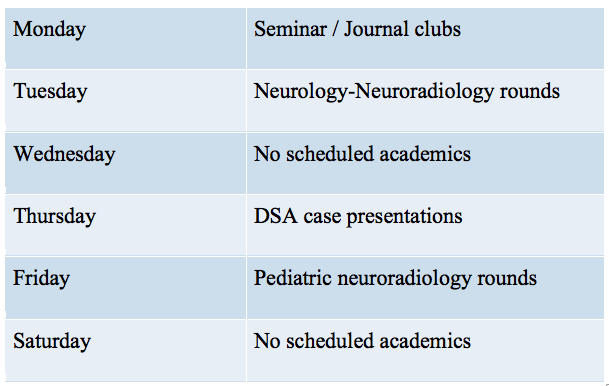
Apart from these classes, there are body intervention rounds every Friday morning and academic activities of the junior residents which can be attended, depending upon your interest and posting.
Duty hours: Though the official timings are 8:00 AM to 8:00 PM, the duty hours vary depending on the place of your posting. The busiest postings are DSA and Trauma centre (CT and MRI).
Regarding night duties: Emergency night duties are on a monthly basis (8 pm to next day 8 am, everyday for a month]. Majority of the calls are from Neurosurgery (CT angio for SAH/ intraarterial nimodipine) and for ischemic stroke from neurology- on an average 4-5 calls per night. The concerned SR is expected to supervise the CT angio, prepare a provisional report and print CT angiogram films without much delay. Along with the night duty SR, the SR posted in the day DSA has to be present for all the mechanical thrombectomies or other major cases done in the night. There is no specific resident room to rest whenever the work is done. But if you are staying in the hostel or near the hospital, it is easy to travel. There are no leaves for the SR posted in emergency duty for the whole month which gets somewhat frustrating at the end of the month. You will be free from night duties roster by the end of fourth semester.
Fee and Salary: The salary structure is Central Govt. Level 11 pay scale as per 7th CPC (same as that of AIIMS/ NIMHANS); so it comes to approximately 90k as of now. Those staying outside the campus get HRA of about 12k. [The exact amount may vary slightly depending on the amount of taxes being deducted].
The annual fees levied by PGIMER is around 8000/-.
Accommodation: Provided in the hostel on campus, depending on the availability. Most of the residents, however, stay outside the campus on rent-based accommodation. You can get rent-based accommodation near the hospital in sector 11 or 15 ranging from 13k to 21k pm, depending on your need.
Leaves: The candidates are entitled for 30 days leave in an academic year and no other kind of leave is admissible to them.
Pros:
- PGI is famous for its bulk of cases. You will get to see a lot of CNS tumours (most of them histologically proven) and almost every form of CNS infection prevalent in India. On an average, you will find yourself reporting 400-600 neuro MRIs/ month.
- Junior residents are available for primary reporting. SRs can sign off the MRI reports. Only doubtful cases are kept for consultant review. It helps to let go routine cases, saving time for discussion of atypical cases.
- Stress-free and friendly environment; faculty and staff members are co-operative and good; everyone shares their experiences. All your questions and doubts will be answered to satisfaction.
- Lots of exposure to head and neck radiology.
- Department is common with General radiology. You can see MSK and Abdominal MRI cases on the departmental PACS if interested.
- You will get to report almost 120-150 CT angiograms per month. You will see almost all vascular variants. Same is true for diagnostic angiograms.
- General radiology postings: PGI has an advantage over other Institutes like AIIMS, and NIMHANS. You can take interventional radiology for various non-neuro vascular and non-vascular procedures. I extended my SR ship for two months to get more hands-on experience in body intervention.
- Exit exams are held at the end of 5th semester- you work like a junior consultant in last 6 months.
- Neuro IR OPD started recently helps to gain some clinical skills, and get follow-ups of prevously treated patients
- Lots of CME’s and conferences: keeps you up to date.
- Lot of exposure to head and Neck intervention cases; more than AIIMS, NIMHANS, JIPMER etc.
Cons:
- Though the Institute has good number of MRI cases, it lacks exposure to advanced imaging tools like fMRI, resting-state fMRI processing etc, although this never bothered me.
- Overall hands-on experience is lesser than AIIMS or NIMHANS. More of first assistant training rather than true hands-on experience (as per personal discussion with colleagues at NIMHANS and AIIMS).
- I feel PGIMER falls behind NIMHANS and Sri Chitra when it comes to academics, especially in diagnostic neuroradiology.
- Language – Not really a barrier; Most of the patients understand Hindi well.
Personal experience: Unlike some Institutes in India, the Department at PGI has a positive work environment that makes you feel good about coming to work everyday and constantly motivates you to give your best effort throughout the day. I got married 2 months before joining PGIMER and I was not sure whether I would be able to get adequately accommodated here. But my academic journey here gave me really good memories to cherish. After my MD, I thought of doing fellowship in Neuroradiology and thus applied for PDCC Neuroradiology at SGPGI, Lucknow. It is difficult to start an academic course of 3 years again after 1-2 years of finishing your MD (especially for radiologists), but the stress-free environment and friendly nature of juniors, colleagues and faculty here never made me feel wrong about my decision. Unlike some Institutes in India, PGI never had any dropouts. Chandigarh is a beautiful and planned city and believe me you won’t realise how the three years just fly off.
Life in Interventional Neuroradiology is exciting, challenging and fun, but can be exhaustive leading to burnout. It might have an impact on your social life as they say “A neurointerventionist is always on call”. Apart from all the stress, neurointervention is not always rewarding as you will see complications that might change the life of patients and relatives, and unexpected outcomes which might add to your mental stress.You will have to face late night studying/ emergency calls, backaches (from the heavy lead aprons), thesis work and examination stress; you have to be on your toes at all the time. However, one thing is for sure, nothing can replace the feel of recanalizing a major vessel in case of stroke or treating SAH patient with altered sensorium and seeing the patients walking and laughing in your follow-up OPD. And as the demand for specialists in radiology is increasing, I would say it is worth doing DM/fellowship courses as per interest.
All the best to the aspiring neurointerventionists. Feel free to contact me anytime in case you have any doubts/ queries.
– Dr.Vivek Agarwal, MBBS, MD, DNB, FRCR, PDCC, DM (PGIMER)
Contact – 7042265309
Email- vivekagarwal0004@gmail.com


Pingback: Radiology Fellowships, DMs and Super-Speciality DNBs in India – Cafe Roentgen
Great post sir. Thankyou:)
LikeLiked by 1 person
Thankyou sir for such a detailed review of the course.
LikeLike