

Duration: Three years.
Number of seats: Since 2019, NIMHANS has started conducting its entrance exam twice yearly – July and January session. The number of seats is as follows:-

N.B: Sponsored seat = service category seat (eg armed forces/ air force/ navy/ govt sponsored candidates. The service category seat may be shifted from one session to the other if no eligible candidates are found
Entrance exams are usually held 2-3 months before the start of the session
Accreditation: NIMHANS being an autonomous body awards its own DM degree. Senior residents need to register with the Karnataka State Medical Council (KMC) after joining NIMHANS for obtaining the KMC registration number. This has been made mandatory by the NIMHANS authorities.
Entrance exam pattern: It is a single step examination (Theory only) comprising of 100 questions — questions will cover all the aspects of General Radiology (MD level) with special emphasis on Radiophysics, Embryology, and Neuroradiology aspects. 1 mark is awarded for every correct answer and 0.25 deducted for every incorrect answer. Since it is a computer-based examination, images of CT/ MRI/ PET-MRI/ DSA will also be there. Based on the theory score, a rank list will be prepared and the candidates will be called for counseling as per merit.
Expected marks for getting a seat:- A score between 70 – 80 might possibly get you rank in the top 3. But you really cannot predict the cut-off as it can vary from year to year.
The marks secured by toppers out of in the past few years are as follows:-

However, there are no MCQ/ question banks to guide you for the DM entrance exam. You can try the FRCR question bank/ MCQs for practice.
Tips on how to secure the fellowship: Know both general radiology (physics and embryology in particular), basics, and theoretical aspect of neurointervention. Get used to basic DSA, SPECT CT, and PET MRI images – a few questions based on images will be there (eg – Moyamoya, Parkinson disease, Epilepsy – FCD, MTS, Aneurysm, stent, flow diverter, CCF and AVM angiography images). Glioma genetics and classification is a current hot topic. The percentage of questions from each of the subspeciality can vary each year but be prepared for questions based on images.
Interventions and Hands-on experience: As the name suggests, the entire intervention caseload in the dept. of Neuroimaging and Interventional radiology (NI&IR) is Neuro. As of now, the dept has a total of 10 faculty members; four of them look into Neurointervention. There are 2 teams [each comprising of 2 consultants] who are posted in DSA every alternate month. The residents are posted in DSA on a rotational basis (the rotation is for 1 month in each modality – CT/MRI/DSA; usually at a time 3 – 4 residents are posted in DSA for one month).
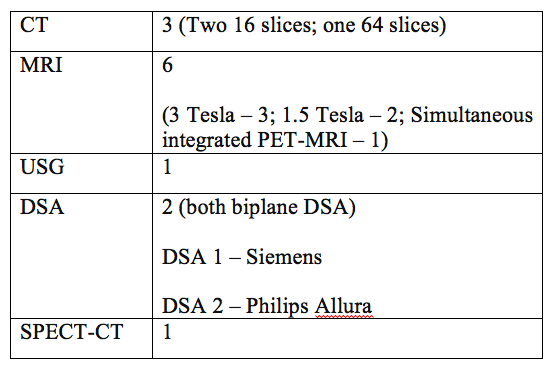
Modalities available in the Department
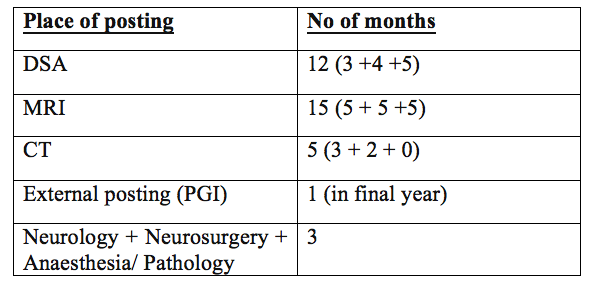
The entire 36 months of DM in NIMHANS are divided approximately as following:
DSA workload:
Diagnostic cerebral and spinal DSA cases (including intra-arterial Nimodipine) – approximately 150 – 200/ month
Neurointervention cases: Varies on an alternate monthly basis (range: 12 – 40/ month); Maximum number of cases that I have seen in my 3-years tenure being done in one month is 42. NIMHANS NI&IR does not have beds on its own – the rights of admitting a patient lie solely at the discretion of Neurologist and Neurosurgeon; which is one of the reasons that despite getting such large number of referral cases – many stable patients roam around for weeks to get a bed; resulting in the reduction of the overall caseload.
In the first 2 years, you get trained in doing all diagnostic cerebral and spinal angiograms. At the same time, you get to assist the seniors and faculty in all intervention cases. Usually by the end of 1 – 2 months, you become confident to do all diagnostic DSAs on your own without requiring the supervision of senior SRs.
3rd year – You do get hands-on – limited number of cases; based on the complexity of a case and depending on the faculty who is doing the case. It remains the final decision of the faculty in –charge whether to allow you to put a coil in an aneurysm or inject Onyx or allow you to do a Mechanical thrombectomy (again varies every alternate month). As for our final year batch, all of us have got more or less equal hands-on under the supervision of consultants. Now as far as I am concerned, I have done 10 mechanical thrombectomies independently (consultant not even entering the DSA cath lab), coiling in 6 – 8 cases, one Glue (NBCA) injection in case of spinal dural AVF embolization, 3 – 4 cases of parent artery occlusion using coils, 2 – 3 cases of Onyx injection, one Middle meningeal artery (MMA) embolization for chronic SDH and innumerable Balloon test occlusion (BTO). How much hands-on you will get varies and will depend on your luck – but you will definitely get a few in your 3rd year.
Academic activities: Morning classes are held daily from Monday to Friday in the Department conference room. All the journal clubs/ seminar/ Topic presentations are done by SRs (on a monthly roster basis) in PowerPoint format. The weekly academic roster is as follows:

The class usually starts at 8:30 am and goes on till 10 am. Once the routine JC/ seminar presentation is over – if time permits, SRs posted in MRI have to show the interesting/ difficult cases for discussion/ consultant opinion. Residents posted in DSA/ External posting are exempted from attending the morning classes. However, they do have to present in case their name is enlisted on the monthly roster.
Apart from the routine morning classes, Neurology- Neuroradiology meets are held daily from Monday to Friday (10 am – 12 pm) in the Departmental conference room. The SR posted in CT is responsible for conducting the Discussion session in the presence of the Consultant in-charge for CT that month.
Every week there is the Epilepsy meet (Thursday 3 pm) – a multi-disciplinary meet comprising of participants from Neurology, Neurosurgery, Neuroradiology, and Neuropsychology. It is usually done by the consultants; as an SR, it is optional for you to attend – if you get time out of your busy schedule.
Duty hours: The duty hours vary depending on the modality in which he/she is posted.

[N.B:- Nuclear medicine is a component of our NI&IR dept itself]
Regarding night duties; Emergency night duties are weekly (9 pm to next day 9 am]. The SR gets a day-off on the very next day. The majority of the calls are from Neuro and Psychiatry casualty – usually for emergency CT findings over the phone (each SR has his/her own personal CUG phone). The major advantage of those living in the hostel is that using NIMHANS net connectivity – institute PACS can be accessed from the room using a laptop. So you can stay in the room at night and answer calls. You need to go only in case an emergency MRI is being done or you are called for an emergency ultrasound. Those living outside the campus can stay in the Departmental Resident room at night.
Fee and Salary: The salary structure is Central Govt. Level 11 pay scale as per 7th CPC (same as that of AIIMS/ PGI); so it comes to approximately 90k as of now. Those staying outside the campus get HRA of about 17-18k. [The exact amount may vary slightly depending on the amount of taxes being deducted].
The annual tuition fees levied by NIMHANS is definitely on the higher side:-
1st year (at the time of admission)– total 70k; 2nd year – 50k; 3rd yr – 50k.
They even charge fees from you for attending your own convocation (Rs. 1975 – in person; Rs. 1000 – in absentia)
Accommodation: Provided in the hostel on campus if required. Two hostels are there:-
Old Kabini hostel – 3 floors; has single as well as married doctors rooms; no separate verandah.
New Kabini Hostel – Newly constructed; 6 floors; single room with bed/table/wall almirah/ mirror/ chair and study table; has attached bathroom and individual verandah. I stayed in the New Kabini hostel for my entire 3 years. Separate hot water taps are provided in all bathrooms; 24 x 7.
Married residents can also stay at the New Kabini hostel. However most of the time, married trainees prefer staying outside within a radius of 1 to 3 km (you can get 1 to 2 bhk rooms/ flats within 15 – 22k).
[N.B – The view from the back facing rooms on the 6th floor of New Kabini hostel is soothing to the eyes]
Leaves: 1st year – 24; 2nd year – 30; 3rd year – 36
Pros:
- Diagnostic MRI – you get a good grasp of pediatric neuroradiology and pediatric metabolic disorders. The major bulk of work on the diagnostic side will be MRI. On average, you will find yourself reporting 400-600 MRIs/ month
- Stress-free and friendly environment; faculty is co-operative and good; no one will scold you and you can interact with them freely
- Hands-on Neurointervention in the 3rdyear
- Plenty of diagnostic angiograms – you will get tired of doing diagnostic cerebral DSAs by the end of your 1 year of posting
- Superb academics – way ahead than AIIMS/ PGI/ SRMC/ JIPMER. Close competition with SCTISMT.
- Exposure to fMRI, resting-state fMRI, and other advanced neuroimaging techniques – for those who are more interested in MRI and neurosciences overall than DSA (personally I never had any interest)
Cons:
- Intervention spectrum – Limited only to Neuro cases
- Neurointervention caseload – Overall on the lesser side (compared to AIIMS/ PGI) since the dept has no beds on its own. Neurologists and neurosurgeons many times refuse admission to NI&IR patients because of high patient load in their own specialty.
- Focus shifting gradually more towards MRI than DSA with 6 MRI machines (a lot of MRI reporting !!!!)
- Language – Not really a barrier; the majority of the patients do understand Hindi (a substantial patient population is from Bengal); for those who do not understand Kannada; the nursing staff and BSc radiography students will be there to act as an interpreter. Learning Kannada is not compulsory. As for my part, even at the end of 3 tears I hardly know anything of Kannada except 6 to 8 words.
Personal experience: 3 years in NIMHANS seem to have passed by in the blink of an eye. This will forever remain as one of the most memorable phases of my life. I have been trying for NIMHANS DM since completing my MD in 2015. In 2015, I was there in the waiting list of NIMHANS but managed to get through PDCC in Neuroradiology at SGPGI, Lucknow. Got a lot of hands-on experience in peripheral vascular intervention besides getting a first-hand taste of neurointervention [However I personally feel 1 year of PDCC Neuroradiology by itself is insufficient to get you the requisite experience and confidence in Neurointervention – You will require a DM or a 2/3-year foreign fellowship to get a grasp of the subject].
Well then came 2016, tried NIMHANS and was again way down in the waiting list, but managed to secure rank 1 in DM Neuroradiology entrance at AIIMS, New Delhi. A few months into the DM course at AIIMS, life started to get bitter and depressing due to the work and departmental environment there. Was looking for an escape path and finally NIMHANS 2017 entrance exam happened. Left AIIMS DM to join NIMHANS in July 2017 and it was a complete game-changer for me. [At present there are 3 residents in our dept. who have left DM at AIIMS to join DM here !!!]
Life at NIMHANS was full of energy, enthusiasm, and a positive work attitude Work, fun, play – a one-in-all. New friends, great department, and overall a friendly working environment, I possibly could not have asked for more. Yes, the stress on MRI reporting is indeed far more than any other institute in India. Hands-on experience in the final year is a huge plus; I got to feel how a microcatheter behaves up there, the first feel of getting to put a coil in an aneurysm, and navigating a guide catheter – you will feel the thrill from within.
But do remember Neurointervention might not always be that rewarding from the patient perspective – it can be extremely unforgiving; one small mistake and you can send an embolus up there in an MCA branch or perforate a small artery in the brain. Sudden unexplained post-procedure deterioration of the patient even after you have a perfect procedure can emotionally and physically drain you. Late night studying/ aching shoulder (from the heavy lead aprons) and odd timing of calls for stroke – you have to be on your toes at all the time. But if you are ready to face the challenge, go for it. Remember – the sky is the limit.
All the best wishes to the aspiring neurointerventionists. Feel free to contact me anytime in case you have any doubts/ queries.
– Dr. Shamick Biswas, MBBS, MD, PDCC (Neuroradiology, SGPGI), DM (NIMHANS); 2017-2020, Former Senior Resident, Dept. of Neuroradiology, AIIMS, New Delhi
Contact – 9945345845
Email- biswasshamick1@gmail.com


Pingback: Radiology Fellowships, DMs and Super-Speciality DNBs in India – Cafe Roentgen
Awesome write up sir
LikeLike
Thank you Dinesh
LikeLike
Thank you
LikeLike
Awesome post . Sir please guide about textbooks, exam pattern of nimhans DM NIR, thesis topics
LikeLike
Hello sir ….
Do you any intervention fellowship program in any indian institute in which DMRD can also / apply / Eligible. .????
LikeLike
My friend has done his 1 yr fellowship in Neurointervention from AIIMS Jodhpur; completed in July 2020. His educational qualifications are MBBS, DMRD, DNB. He got into the fellowship post DMRD. However whether u can apply for fellowship in a Govt set up after DMRD directly – I am not sure; U need to check for the eligibility criteria when these advertisements are made.
For a fellowship rom a Pvt set up like Mumbai , Delhi, Bangalore and Coimbatore (etc…) — U can check the websites if you are eligible
LikeLike
Sorry for the typo error — He got into fellowship, after completing his secondary DNB from Delhi
LikeLike
Thank you for the article sir, could you advise a book to read neurointervention from?
Also, if you could comment on career prospect and job availability in body vs neurointervention.
Thanks.
LikeLike
Book wise – osborn, neuro portion from aiims mamc pgi imaging series and possibly frcr mcq books for practice
regarding job and future prospects — neurointrvntn has a steeper learning curve, cost is pretty much on the higher side
body intervention – shorter learning curve, patient outcome may b much better and less costly
dont worry about jobs – whichever field u choose to pursue, learn it well — u need to invest time to succeed
LikeLike
Thank you for such an amazing article.
Reading Osborn is enough or have your read Scott too ?
LikeLike
osborn is enough for ur DM entrance exam — to be true to u, even i havent read scott during my DM 😂😂
Osborn n berry series should suffice, add to that radiopedia and journal articles (if possible)
LikeLike
Hello sir..thanks for that really inspiring and detailed write up.. Could u pls shed light on the work life balance post residency in inr field? I cant do 48hrs on call even after residency.. Can I practice in a way that I do diagnostic for 3 days and neurointervention for 2 days (money is not a priority. Im ok with lesser earnings). Is there a practical scope for striking such a balance in india? Thanks in advance:)
LikeLike
Hi nice readingg your post
LikeLike
Thank u for such wonderful writing. Can you give insight of the job opportunities & role in corporate hospital (Only Intervention or both diagnostic and intervention) after DM Neuroradiology & NIR ? Because now those trained with 1 year IR fellowship also doing head to toe including Neurointervention, Neurologist & neurosurgeon also doing Endovascular procedures.
LikeLike