

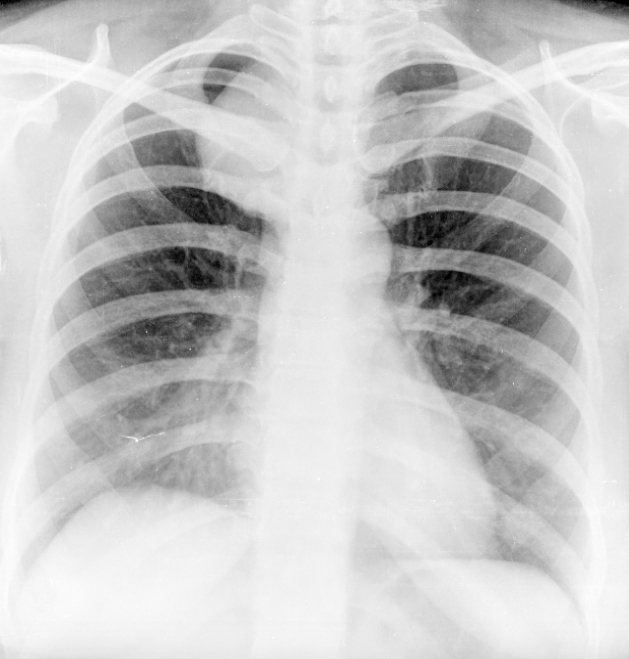
This is a frontal chest radiograph (do not state AP or PA in exams nor talk about well-centralized or rotated unless you are prepared for the viva to go there!).
There is a well-defined homogeneous 5×3 cm vertically oval soft tissue lesion (in practice, prefer stating ‘lesion’ or ‘shadow’ over ‘mass’, especially for benign findings, as patients are scared to hear the word ‘mass’, which is often taken synonymous for malignancy) in the right paratracheal region along the lower third of the trachea (notice how this description states the location of the lesion without getting into whether this is pulmonary or mediastinal and where in the mediastinum). There is no calcification or cavitation present. The superior and lateral borders of the lesion are well seen, indicating that it lies within the posterior mediastinum (cervicothoracic sign). Adjacent bones are normal with no scalloping, nor is there any widening of the intervertebral space.
The right dome of diaphragm is elevated. Most commonly, this would be a normal variant. However, given the presence of the aforementioned lesion, there is a slight possibility that this is secondary to right phrenic nerve palsy. Mild congestion is also present in the right lower zone, which may be secondary to this. The lungs are otherwise clear. Both the CP angles are normal. Cardiac shadow is normal. The upper abdomen and rest of the bones are normal.
Given these findings, the most likely differential is a neurogenic tumor (prefer this term to PNST, as it encompasses more lesions). Other differentials include a duplication cyst (which is statistically much rarer but may present with a similar radiological appearance), and an aneurysm (unlikely).

On CECT, there is a well-defined lesion, closely abutting the trachea and esophagus; suggestive of a foregut duplication cyst.
Thus, this is actually turned out to be one of the zebras! In majority of the cases, the correct diagnosis would be a neurogenic tumor, given the rarity of posterior mediastinal duplication cysts. The lack of widening of the intervertebral spaces was perhaps a clue, but can often be absent even in neurogenic tumors.
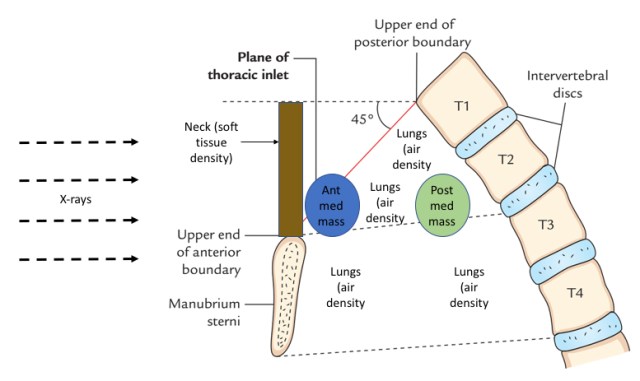
Cervicothoracic sign: This was also discussed in the Dr Bhavin Jankharia’s recent talk (great minds think alike!). The sign was described by Benjamin Felson and is a corollary of the silhouette sign, and can be applied to soft tissue density masses. The anatomic basis for the sign is the obliquity of the thoracic inlet (remember this term and state this if asked in your exams). The thoracic inlet is bounded by T1 vertebral body posteriorly, the first ribs on both sides, and the superior border of the manubrium anteriorly.

https://www.earthslab.com/anatomy/superior-thoracic-aperture-thoracic-inlet/
Thus, at the posterior aspect, the thoracic inlet is higher up, and the lungs thus are present superior to the level of the clavicle. Hence, any posterior mediastinal mass will be surrounded by lung tissue laterally and superiorly. Given that it is a soft tissue density mass, we will see a sharp demarcation between the mass and the air-density lungs, and thus the superior border of the mass will be appreciable above the clavicle as well.
On the other hand, at the anterior aspect, a soft tissue density mass in the mediastinum would merge with the soft tissue density of the neck anteriorly as there is no interim air-density lung parenchyma to provide a silhouette. Thus, the superior border of the mass will not be appreciable above the clavicle in an anterior mediastinal mass.
The below figure may help understand this better.
– Akshay Baheti, Tata Memorial Hospital

Awesome… Wish to have more n regular lectures by such great facultys 😊😊😊😊😊
LikeLiked by 1 person
this explanation is easy…worthy to remember easily..thnx…need more more lectures…
LikeLike
Superb teaching points..
LikeLike
Very nicely explained
LikeLike
Well explained, thank you sir
LikeLike
simply too good.
LikeLike
Well explained
LikeLike
Excellent. Thank you sir.Need more explanation like this in common topics/signs.
LikeLike
Thank you sir. Listening to your classes have always been a pleasure.
LikeLike