

After discussing how to write a good impression in the previous blog, I will now talk on how to describe findings succinctly but completely. Apart from discussing some basic rules in brief, I will again give examples of how I would describe a particular finding to make it more practical.
1. As discussed in the blog on Anatomy of the Radiology Report, the findings section of the report is where we described what we see. The description should be such that the referring physician can mentally ‘see’ the actual image on reading our description. To use an RR aphorism, a man sitting on the moon should be able to hear the report and ‘see’ the image.
For example, does this description gives you the best picture of the lungs in this patient with metastatic cancer?
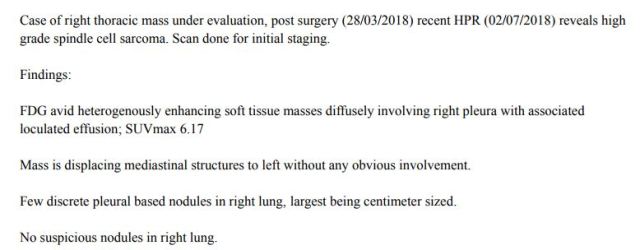
For a complete picture, we would need a fair idea about the size, number, and location of the metastases, which is lacking here. Here is how I would instead describe multiple pulmonary nodules.
‘There are multiple (at least 10) bilateral lung nodules, largest measuring 1.5×1.3 cm in the right upper lobe, consistent with metastases.’
or
‘There are a few (at least 4) bilateral subcm non-calcific lung nodules, largest measuring 6 mm in the right upper lobe; these are indeterminate and should be followed up in 3 months with a non-contrast CT chest to rule out metastases.’
I use this as my stock phrase for most descriptions of ‘multiple’ observations (like lung nodules, hepatic lesions, etc). I always qualify the word ‘multiple’ with ‘at least x’ to give the doctor an idea of the number of nodules (it can be ‘at least 4’ or ‘at least 10’ or ‘>20’ or ‘innumerable’). I usually do not count the exact number unless it is less than five nodules, but give a rough guestimate depending on what I see. And then I give the size (and perhaps location) of the largest observation. I add a short comment on the presence of calcification/cavitation if I see it. Such a description incorporating size, location, and number will give a good mental picture to the referring physician about the image.
2. Although you need to describe everything well, the description of the findings must be as short as possible. Generally, the length of the report is inversely proportional to the confidence of the reporting radiologist! Watson and Crick’s seminal paper on the structure of DNA (in which they described the double helix model) is.. hold your breath.. 900 words long! Certainly, if they can describe the double helix model for the first time ever in about 900 words, we can try to keep our reports short and yet convey the findings without complaining!
To achieve this, try to create your own phrases to shorten descriptions without losing information. For example, instead of saying that ‘There is a 7 mm calculus in the right renal pelvis. No hydronephrosis or hydroureter’, you can say ‘There is a 7 mm non-obstructive right renal pelvis calculus.’
In a similar vein, avoid repetitive words:
‘the lesion is small in size’ can become ‘the lesion is small’ or simply ‘small lesion’;
right middle lobe or left lingula is a tautology, as the middle lobe is always on the right and lingula on the left;
‘causes mass effect in the form of compression of the adjacent IVC without occlusion’ can become ‘compresses the adjacent IVC without occlusion’.
3. More tips for a faster and more concise description.
a. Do not give detailed descriptions for incidental findings of no import (e.g. simple renal or hepatic cyst) or findings expected at the patients age (e.g. degenerative changes in the spine on a CT abdomen pelvis or age-appropriate chronic microvascular ischemic changes in the brain). While most radiologists do want to comment on such non-specific findings in the findings section (to avoid any allegations of ‘missing something’ or any potential medicolegal issues), remember to never put such findings in the impression, nor bold or italicize them.
b. Do not describe the imaging findings in detail for pathognomonic findings (for example, say ‘there is an acute non-hemorrhagic left frontal MCA territory infarct’ rather than ‘there is a wedge-shaped hypodensity in the left frontal region involving the grey and white matter, consistent with an acute left MCA territory infarct’).
c. How many incidentals or anatomic variations should you report? Everyone has his own view on this. Some would report every splenunculus or focal fatty change along the falciform ligament, while some would let these go. Just follow what you feel makes sense. Either ways, you should keep the description short. So nothing more than a ‘Small splenunculus incidentally noted’, if you report it at all. I would use something similar for incidental benign lesions of no import. So I would write ‘1.8 cm right hepatic hemangioma noted’ rather than ‘There is a 1.8 cm seg VI lesion demonstrating peripheral discontinuous nodular enhancement with centripetal filling in, consistent with hemangioma.’
4. Avoid the passive voice as much as possible; the active voice usually has more impact. To again give Watson and Crick’s example, they start the paper by stating ‘We wish to suggest a structure for the salt of deoxyribose nucleic acid’; active voice! Active voice exerts confidence and the willingness to take responsibility for what one is saying. So, prefer describing an observation as ‘There is a right lung mass…’ rather than ‘A mass is seen in the right lung…’
When would it be better to use the passive voice? In instances where you do not want to give a lot of importance to the findings. So I will often use passive voice for incidental or unimportant finding – ‘few bilateral simple renal cysts incidentally noted’ or ‘tiny left upper lobe calcific granuloma seen’.
5. Grammar is important! You read the report of any prominent radiologist, and it will almost never have poor grammar. The best radiologists are grammar Nazis in a sense. Their report will also contain certain set phrases and terms, which can be clearly seen as painstakingly created and perfected over a lot of time and thought.
Wording the report is an expression of what you think and who you are. The very act of deliberating about how to word a report appropriately makes you think more about the findings and their importance with respect to the patient’s management, and helps understand the findings better. So over time, make it a practice ponder over words just like you ponder over findings. Also read other good radiologists’ reports carefully, and then amalgamate the best of your thoughts and others’ examples to create your own style of describing various common abnormalities and findings.
For example, I often see collapsed bowel loops which appear thickened, and feel that this thickened appearance is most likely due to the fact that the bowel loop is not distended. So I use a phrase ‘apparent thickening of the collapsed colon, likely due to underdistention’ and bury this in the findings without mentioning it in the impression.
Similarly, many radiologists go on and on describing post-operative findings, none of which are out of the ordinary. In such a case, I prefer using the term ‘expected post-operative changes noted’, and describe these in brief if required.
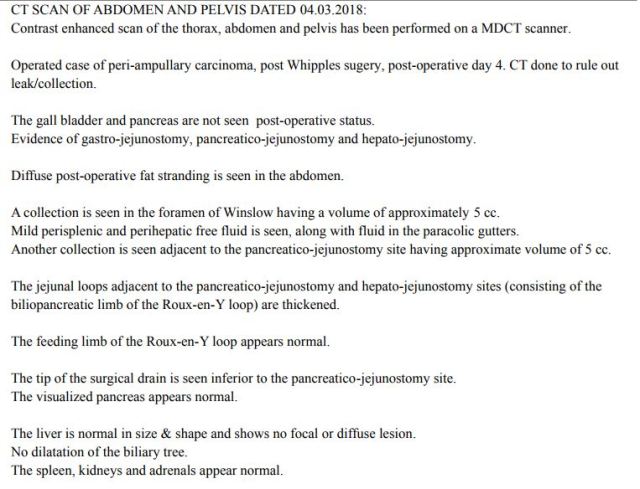
For example, look here at the detailed description of the post-op findings by my sincere resident. I would instead just state ‘The patient is status post Whipple’s procedure, with expected post-operative findings. The post-operative drain is in appropriate position. Small 5 cc collections present in the foramen of Winslow and near the pancreatico-jejunostomy site. Mild perihepatic and perisplenic fluid, within expected limits. No other collection.’
6. Avoid hedge words (these are non-committal or ambiguous words) as much as possible. Although we cannot remove them from the report completely, a good rule of thumb is to use them in less than 10-20% of all sentences. Examples of hedge words include ‘no obvious abnormality’, ‘no appreciable abnormality’, ‘there appears to be’, ‘no definite nodule seen’, ‘essentially normal study’ etc. In each of these examples, the meaning of the phrase does not change even if we remove the hedge word; however the hedge word makes us sound more evasive and commitment phobic. Radiologists are in fact nowadays so infamous for hedging that Dr Hemant Morparia, a reputed radiologist and equally reputed cartoonist, created a cartoon for us showing a hedge-fund manager who subsequently becomes a radiologist! We published this cartoon (amongst seven others that he created for us) in our book on Practical Radiology Issues co-written by me and Dr Bhavin Jankharia in a chapter on reporting.

7. Do not use the phrase ‘evidence of’ except in appropriate instances; this is a very Indian (or at least Mumbai) thing. If you see a renal mass, say that ‘there is a renal mass’, and avoid stating ‘there is evidence of a renal mass’. Use ‘evidence of’ when you wish to summarize something in the impression, such as ‘No evidence of metastatic disease in this patient with renal cancer’, indicating you have searched everywhere and have not found any suspicious lesion in the patient. For the body of the report, a good example of when to use this phrase would be to say ‘There is cholelithiasis without evidence of cholecystitis’ instead of saying ‘There is cholelithiasis. No wall thickening. No fluid or fat stranding around the gall bladder to suspect cholecystitis.’ Dr Ravi Ramakantan explains this beautifully in his blog on the language in the radiology report.
8. Describe relationships of a mass clearly. I often see reports talking of masses abutting adjacent organs without clarifying whether this means invasion (T4 stage disease) or not.
For example, ‘there is loss of fat plane between the cervical mass and the posterior wall of the urinary bladder’ doesn’t clarify whether the mass is involving the bladder or not. Add an additional phrase ‘No invasion’ or ‘No obvious invasion’ (it is OK to use a hedge word here as we cannot rule out microscopic invasion).
9. Create your own search patterns and set phrases when you describe common abnormalities. This will save time, and will also ensure that you do not miss out on a description. For example:

‘There is an enlarged right paracaval node compression the mid ureter, with mild proximal hydronephrosis and hydroureter and a delayed right nephrogram. No renal atrophy.’
Thus, in any case with hydronephrosis, I always comment on the site of obstruction (distal/mid/proximal), severity of obstruction (mild, moderate, or severe hydronephrosis), presence of symmetric or delayed nephrogram, and presence or absence of atrophy (especially in patients with a delayed nephrogram).
Another example in a patient with bone metastases.


‘Diffuse mixed lytic-sclerotic vertebral and pelvic metastases seen. There is an approximately 70% compression fracture of the D4 vertebral body. No soft tissue component.’
Thus, in every case of vertebral metastases, I talk on the presence of absence of a compression fracture. If it is present, I talk about the severity of compression (mild, moderate, severe, or better still a percentage), and state whether there is associated soft tissue component (particularly epidural soft tissue component). Describe benign osteoporotic compression fractures similarly.
10. It is a good practice to give image numbers in the report for important or subtle findings. For radiologists using PACS, this is very easy. For those providing films to patients, you can still certainly give the film and image number. It makes life very easy for other radiologists or referring physicians trying to understand the report. We in Tata for example often have to spend a long time trying to search for tiny lung nodules reported in an outside study, as the image number is not provided. Marking on the films is something which has varying opinions; some referring physicians like it while others feel it may obscure some other important finding, and so giving the image number is probably better.
In a similar vein, some radiologists also bold or italicize positive findings. This is not a uniform practice and has its pluses and minuses. Either ways, if you do want to do this, be sure to do so only for positive relevant findings, and not for all non-specific findings as well.
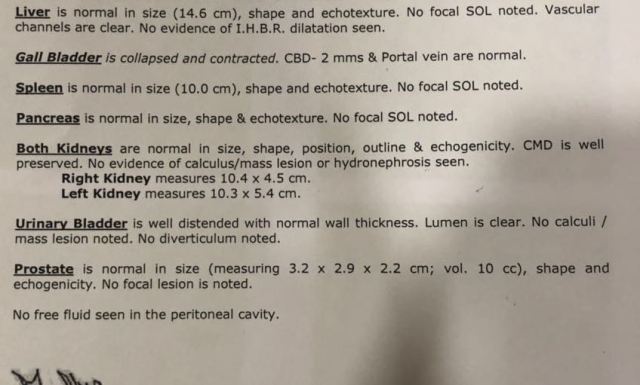
For example, this was my nephew’s completely normal USG abdomen report (he had hepatitis). Not only was there no impression stating that this is a normal abdominal ultrasound, the radiologist also italicised that the gall bladder is collapsed and contracted. His parents freaked out thinking this is something abnormal, and immediately called me to clarify. It took me some time to convince them that this was normal, as they couldn’t understand why would this finding be in italics if it was normal!
For last words, a few general statements on some common words which you should or should not use (in my humble opinion of course!)
i. Lung fields are clear: have you ever used terms like ‘kidney fields’ or ‘liver field’? Just say ‘Lungs are clear’ please!
ii. Bilateral vs both: always confusing on when to use what. I would say ‘Both lungs are clear’ or ‘Lungs are clear bilaterally’.
iii. Conglomerated nodes or conglomerate nodes? I would use conglomerate; another word I often use instead is confluent nodes.
iv. Visualized vs seen: Technically, visualizing is used more in the sense of imagining than seeing (you visualize a swachh Bharat but certainly don’t see it!). So avoid saying ‘mass is visualized’; it should be ‘mass is seen’ (or better still ‘there is a mass’)!
v. Mass lesion: This is often used by the residents in Tata at least. Use either ‘mass’ or ‘lesion’; mass lesion is a tautology.
vi. Proximal IVC or distal IVC?: This is always confusing when describing veins or ducts, as the anatomic ‘proximal’ does not match the physiologic ‘proximal’ in terms of flow. I hence prefer using the words ‘upstream’ and ‘downstream’ instead; there is no scope for confusion. Upstream IVC or downstream CBD can only mean one thing!
I am sure there are many other opinions on what I have written, as also many things I have missed writing upon. Do share what you feel on how to report findings by leaving your comments and opinions in the comments section.
– Akshay Baheti, Tata Memorial Hospital

Great read!!! Thanks for sharing such a great blog.
LikeLike