
Every radiology report should (and usually does) have a basic structure to it, particularly for CT and MRI reports. Radiologists generally follow this structure as a regular template, or sometimes may follow parts of it subconsciously. But a good way to start our ‘reporting series’ is to discuss the basic structure or the anatomy of the radiology report, which all of us are aware of, and discuss some basic concepts and details.
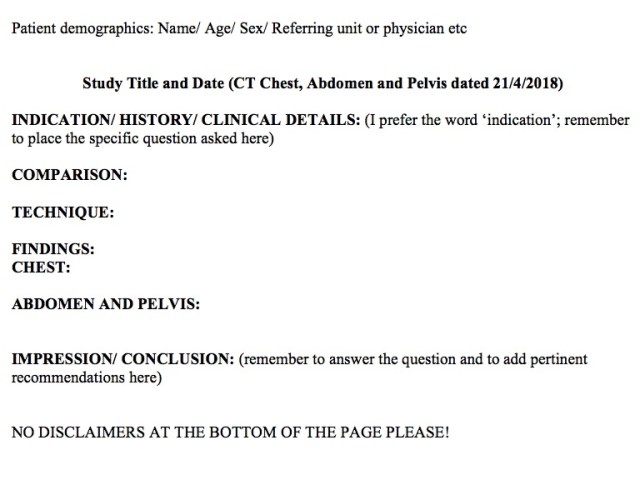
Patient demographics, and title and date of the study: Self-explanatory; every report has this incorporated. We will take a CT Chest, Abdomen and Pelvis (CAP) dated 21st April, 2018 for a patient with colon cancer as our stock example.
Indication/ History/ Clinical details: The clinical picture of the patient is written here. This is extremely important; to use an RR aphorism, ‘a good history is worth a thousand images’. I personally prefer the word ‘Indication’ to history or clinical details. This is because, literally, ‘indication’ means the precise reason why the study is being conducted; the question which needs an answer. It is more specific than ‘history’.
For example, a CT CAP may be performed for a patient with ‘history of colon cancer’, but the indication may be ‘post right hemicolectomy with fever; rule out collection/infection’ or ‘Colon cancer; surveillance scan’.
Ancillary details and pertinent negatives should be noted here; for example, ‘Colon cancer; surveillance scan. Tumor markers are normal’. Say for a different patient with a CT chest, indication may read ‘Gradually progressive breathlessness and cough; chronic smoker; weight loss present’ or ‘Gradually progressive breathlessness and cough; non-smoker; has exposure to pigeons’.
Comparison: This is something often missed, especially in imaging centers where prior imaging is not always easily available compared to hospitals. Remember the words of Benjamin Felson: ‘The world’s greatest consultant to a radiologist is a patient’s previous imaging studies’. It is important to demand prior imaging (if it has been performed) in all patients, and train the receptionists and technologists to insist on asking for these from the patients. This is particularly important for chronic conditions like cancers and interstitial lung diseases. Rarely, you may need to compare with multiple priors as well. Examples:
‘Compared with previous CT CAP dated 21st October, 2017’; or
‘Compared with previous CT Chest dated 11th January, 2018, and CT CAP dated 21st October, 2017’ (Our hypothetical colon cancer patient might have had an interim additional CT chest to follow an indeterminate pulmonary nodule); or
‘No previous imaging available for comparison’
Technique: Different institutes and imaging centers may describe the scan technique in varying details, including details of the primary scan and the reconstructions. For an MRI, details of say perfusion and spectroscopy may also be described in varying details. Stick to your institute’s policies. However, some important points need to be borne in mind.
i. IV contrast is a prescription medication (as radiologists, WE legally prescribe contrast and not the referring physician, and we are responsible for maintaining its records). Hence, details about contrast administration need to be included. Ideally, the actual dose of contrast injected should be mentioned (as is always done in the US), but at least the specific contrast used should certainly be mentioned. This is good practice, especially in MRI, given that macrocyclic agents have less Gd deposition in brain compared to linear agents; such things must hence be there in the patient records as it may be potentially needed in the future.
ii. Any additional or non-standard sequence/ procedure must be mentioned. Examples: ‘Hepatobiliary phase MR images were obtained at 2 hours’; ‘Marker was put over the site of the patient’s ankle pain prior to beginning the MRI study’; ‘Oral contrast was given on table to distend the esophagus in this patient with suspected esophageal mass’; ‘Rectal contrast was administered prior to the study’
iii. Any adverse incidence must be mentioned, either here or later after the impression. Examples: ‘Patient developed mild contrast reaction in the form of hives after the contrast administration, which was treated with Benadryl’; ‘Approximately 20 cc of contrast extravasation occurred, with the patient having no symptoms. ‘Venous’ phase images are slightly delayed because of this reason.’
Findings: This is the body of the radiology report, where we describe what we see. The description can be completely free text (starts with positive findings and then negatives/normal in short), or can have some structure to it. I find having at least some structure in the findings section makes the report more readable. So the minimum I put in my reports is a separate ‘CHEST’ heading and describe all chest findings there, and a separate ‘ABDOMEN AND PELVIS’ heading and describe all abdominal findings there. Others (especially in the US) have a report similar to a USG report; i.e. separate lines for comments on liver, spleen, gall bladder, pancreas, kidneys etc. I find this very useful as well, especially for training newly joined residents to develop a comprehensive search pattern. If I had my way, I would make all my residents use this format, as I learnt a lot this way in terms of not missing subtle findings during my US stint. Bottom line is that all three formats are fine to use; the important thing is to miss nothing and describe the findings appropriately in a way the referring physician and patient are comfortable reading.
Different radiologists have different approaches on how much detail to report. Some wish to report everything they see, while others would rather not mention the incidental splenunculus or a small simple renal or hepatic cyst. We will get to the pros and cons of either approach in a separate blog later.
What is important though is that we precisely describe pathology in a way that the referring physician can mentally ‘see’ the actual image on reading our description. To use another RR aphorism, a man sitting on the moon should be able to hear the report and ‘see’ the image. We will discuss multiple examples of this in subsequent blogs.
Finally (although this may sound counter-intuitive), the report must be as short as possible. A long winding report does no good to anyone, and is usually unreadable. Remember Mark Twain’s famous words ‘I didn’t have time to write a short letter, so I wrote a long one instead.’ Every patient deserves the time and thought that goes into making a short, concise, and complete report.
Impression/ Conclusion ± recommendations: While we describe what we see in the findings, we describe what we think in the impression. Most importantly, we answer the question (the indication) with which the referring physician referred the patient for the study.
Do not copy paste all findings and put them as the impression; the two sections have different purposes. No one enjoys reading a 20 line long impression anyway; it has to be concise.
The impression also needs to be clinically relevant. So, in a patient with metastatic colon cancer, an incidental gall bladder or renal calculus should be mentioned in findings but not in impression. I prefer writing the impression point wise for better readability if there are more than 2-3 findings.

Our job does not end here; we must also make relevant recommendations when needed. I have realized that this is what residents miss out on the most; they forget to include these in an otherwise excellent report. Some radiologists prefer using the word ‘suggest’ instead of ‘recommend’; also equally valid. The word ‘advice’ is perhaps less suited, as the referring physician hasn’t asked for our advice but for our opinion. Remember that if you are recommending follow-up, give a time frame for the follow-up.
An example of impression in our hypothetical colon cancer patient will be (assume the patient has been treated and this is a surveillance scan):
Situation A: No prior imaging given for comparison.
‘CT study reveals:
- Indeterminate 3 mm right upper lobe pulmonary nodule.
- Status post right hemicolectomy. No definite recurrent or metastatic disease.
Comparison with the patient’s prior imaging is needed to evaluate for the temporal stability of the pulmonary nodule. Alternately, a 3 month follow-up CT chest is recommended.’
Situation B: Prior imaging available for comparison.
‘CT reveals a single new hepatic lesion, consistent with metastasis given the increasing tumor marker levels. No other suspicious lesions seen. USG-guided sampling can be performed for confirmation.’
To read the 10 golden rules on how to write the perfect radiology impression, read our blog here.
A note on disclaimers: I often see outside reports giving silly disclaimers at the bottom of every report like ‘This is just an opinion and has no medicolegal validity’ or ‘This is just an opinion and not a diagnosis, and needs to be correlated with clinical and laboratory parameters’. These are plain stupid and are anyway not going to protect you from a medicolegal case if it comes to that. Otherwise every doctor would have started putting such disclaimers on all OPD and inpatient papers. You will not hear of such disclaimers even in the US, the most litiginous country in the world! Refrain from putting any such disclaimers.
– Akshay Baheti, Tata Memorial Hospital

Pingback: ‘Whats your impression, doctor?’ A guide to writing the perfect radiology impression – Cafe Roentgen
Pingback: The Art and Science of Radiology Reporting – Cafe Roentgen
Pingback: The Findings (Body) of the Radiology Report: What to say and how to say it? – Cafe Roentgen