

We often come across incidental abdominal aortic ectasia or a splenic artery aneurysm while reporting a CT and wonder what to do about it. The ACR gave useful recommendations for their management in 2013, in a closed-access paper available here.
Unlike other white papers, the white paper on vascular findings does not give a lot of flowcharts or tables. However, we list some of its salient recommendations.
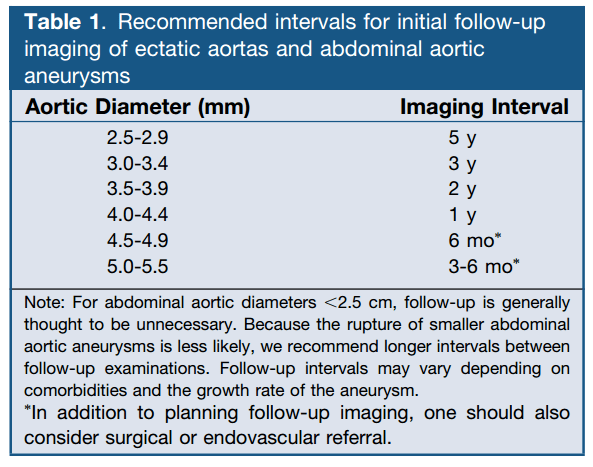
1. Follow-up Interval for Incidental Abdominal Aortic Ectasia/ Aneurysm
2. Penetrating aortic ulcer: The ACR recommends annual follow-up for asymptomatic penetrating aortic ulcers, and more frequent follow-up if symptoms are present, with consideration for surgical or endovascular intervention.
3. Iliac artery aneurysm: Iliac artery aneurysm is defined as a vessel diameter 1.5 times the normal iliac artery diameter or 2.5 cm in diameter. Aneurysms <3.0 cm in diameter are usually asymptomatic, expand slowly, and rarely rupture, and need not be followed up. Aneurysms between 3.0-3.5 cm should be followed up initially at 6 months. If stable, further follow-up can be performed annually. Aneurysms >3.5 cm have an increased tendency to rupture and should be treated or followed more closely.
4. Splenic artery aneurysm: Annual surveillance is recommended. Surgical literature suggests a consensus that such an aneurysm should be considered for endovascular therapy when ≥2 cm. Surveillance intervals of >1 year may be reasonable for the smaller aneurysms, depending on comorbidities and life expectancy.
5. Renal artery aneurysm: The ACR recommends an imaging follow-up in
asymptomatic individuals every 1 to 2 years. Larger aneurysms, measuring1.5-2.0 cm or more, should be considered for surgical or endovascular repair.
– Akshay Baheti, Tata Memorial Hospital
PS: All images are a copyright of the original published article.

Pingback: Incidental Findings Follow-up Recommendations – Cafe Roentgen