

There are two separate criteria for incidental lung nodule management. The more commonly used one is the Fleishner criteria, last updated in 2017.
Note that the Fleishner criteria can not be applied to patients with known primary cancer, patients with immunosuppression, patients <35 years age, or to lung cancer screening, and need slice thickness ≤1.5 mm. There are different criteria for solid and subsolid nodules.
Assigning a patient to low vs high risk is slightly more difficult now than in the old versions of these guidelines. In general, high risk factors include history of heavy smoking, older age, irregular or spiculated margins, larger nodule size, and upper lobe location, while low risk is vice versa. Do read the open access Radiology 2017 article here for more details.
Follow-up of solid nodules:
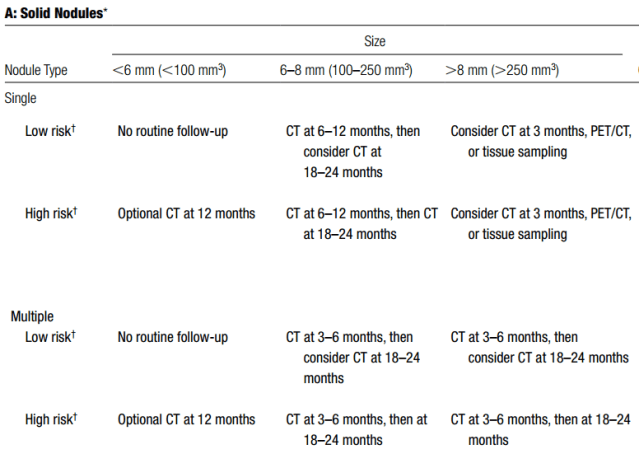
Note: For multiple nodules, use the most suspicious nodule to guide management. Follow-up intervals can be varied depending on the size and risk of the nodule in cases where there is a follow-up range recommended.
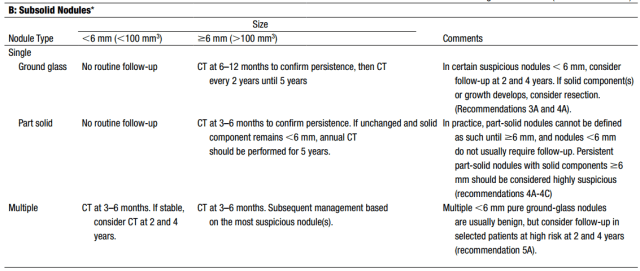
Follow-up of subsolid nodules:
The less commonly used LungRADS is specifically used only in lung cancer screening and is available at the ACR website. We are not putting it up here as it is quite detailed and is useful only in a small subset of patients. If you perform lung cancer screening CTs, I would suggest keeping a printout handy, or downloading the pdf and keeping it on your cellphone/tablet.
– Akshay Baheti, Tata Memorial Hospital
PS: All images are a copyright of the original published article.

Pingback: Incidental Findings Follow-up Recommendations – Cafe Roentgen