

The question mark (or ‘query’ as we call it) is commonly used in medical lingo and formal medical notes; we constantly use it to denote a possible diagnosis. For example, medicine residents may write in their notes ‘History of fever, cough, and weight loss for 2 months; ?Kochs’, and then would present the patient to their consultants as ‘This is a patient of query Kochs’. Possible Kochs would perhaps be more appropriate grammatically while presenting, but somehow the word ‘query’ is ingrained in us as medical students, as this is how we write our notes in MBBS days.
Using the ‘query’ in medical notes is perhaps acceptable as this is mainly meant for other medical practitioners and everyone would understand this lingo. Unfortunately, this term has insidiously made its way into the radiology report as well. I use the word unfortunately as the ‘query’ is often used very loosely in the report, and impressions labeling a lesion as ‘?nature’ or ‘?neoplastic’ or ‘?benign ??neoplastic’ (!) abound.
For example, a distant relative of mine, a 50-year old gentleman, recently underwent an upper GI scopy for symptoms of gastritis. The scopy found a small duodenal nodule, which came out to be a well-differentiated neuroendocrine tumor (grade I NET with MIB1 index of <1%) on biopsy. This was felt to be an incidental finding (these are leave alone lesions). However, a somatostatin scan was performed to confirm that this was localized disease. Here is the final impression given in the report.

The radiologist describes that known primary duodenal nodule does not show somatostatin uptake. However, there is mild uptake described in a portocaval node, and then the radiologist adds the ‘query’, labeling it ‘?metastatic’. Most of us will find it a very reasonable description, but pause and think from the patient or the referring doctor point of view. If the node is not metastatic, the patient does not require any treatment or even surveillance. However, if it is metastatic, he will require a Whipple’s surgery, with a 3-5% risk of death and a 25-30% risk of morbidity! And the radiologist has not given any differentials, nor stated what s/he feels actually about the node. Query by its definition indicates uncertainty rather than certainty, and whether there is a 50-60% chance of the node being metastatic vs a 70-80% chance vs a 20-30% chance makes a big difference. The single ‘?metastatic’ is a very incomplete description indeed!
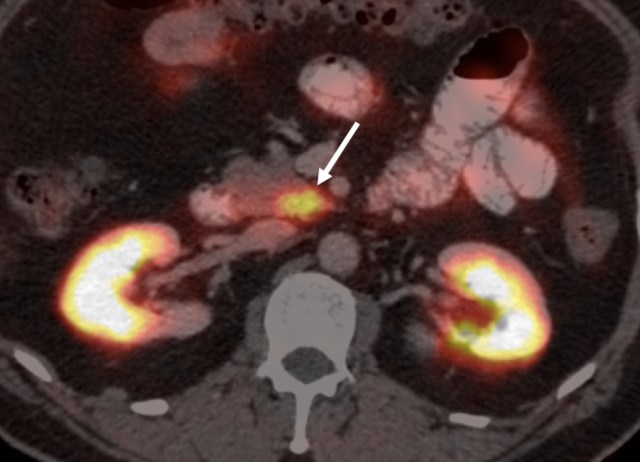
A better worded impression (particularly considering that the pre-test probability of it being metastatic is very low) could have been ‘there is mild uptake in a single portocaval node, which may be physiologic and benign, although metastasis remains in the differential’. Luckily, the relative shared the scan with me and our nuclear medicine dept quite categorically stated that the purported nodal uptake was actually physiologic uptake in the uncinate process of the pancreas. The ecstatic patient was supremely thankful, and is leading a normal and healthy life since then.
I can share multiple more examples (refer to my blog on How to write the perfect Impression (point 6) for another one), but essentially, somewhere along the line, radiologists have started using the term ‘query’ very loosely in radiology reports. The ‘query’ is now more often than not used as a hedge; an escape route to refrain from committing to a diagnosis or a reasonable set of differentials in the order of likelihood. It actually often stops the radiologist from thinking further and phrasing a much better and clearer impression.
What can we do instead then to convey our certainty or uncertainty better? Radiology actually already has a beautiful lexicon in place in certain specific cases precisely for this; namely BIRADS/ LIRADS/ PIRADS. So for example BIRADS I is normal, BIRADS III is indeterminate, and BIRADS V is highly suspicious for malignancy. Referring physicians love these lexicons, and indeed in many cases the management strategy is defined by what is the lesion’s BIRADS or LIRADS category. Some of us in Tata have created a similar lexicon for communicating certainty, taking a cue from our colleagues in MSKCC (read their approach here). We now use this lexicon at the end of every report, and use the precise terms in the lexicon for describing every relevant lesion.
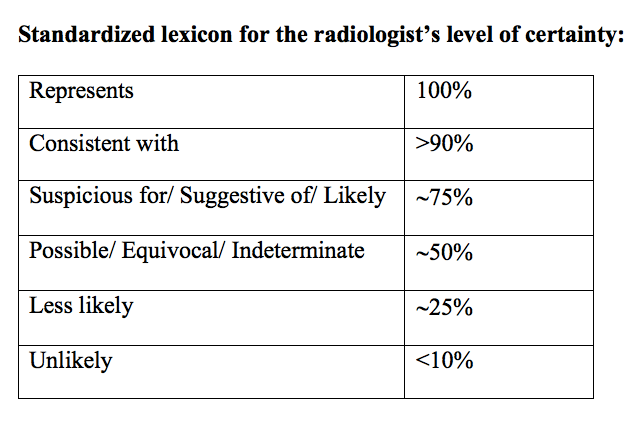
For example, a sclerotic bone focus seen in a patient with pancreatic cancer at baseline staging scan can be called as ‘unlikely to be metastatic’ or ‘consistent with bone island’ if one believes it is benign. Similarly, a 3 mm lung nodule in a patient with colon cancer would be called ‘indeterminate’, a 7 mm nodule in a similar patient would be ‘suspicious for metastasis’, while a 13 mm nodule would be ‘consistent with metastasis’ or ‘represents metastasis’.
For the report discussed above, the reporting person could have stated ‘equivocal for metastasis’ or ‘indeterminate in etiology; metastasis is in the differentials’, or could have stated ‘less likely to be a metastatic node’ depending on his/her level of certainty. The radiologist can decide which descriptor to use; but the level of certainty is conveyed clearly. The ambiguity of the ‘query’ or the ‘possible’ or ‘probable’ or ‘suspicious for’ goes away, as these terms may otherwise be interpreted differently by different people. Also, I believe this is medicolegally very safe, as (apart from ‘represents’) there is always some scope left for a different diagnosis than the one we commit to. Thus, using this lexicon is in the interest of the patient, the referring physician, and the radiologist as well!
In conclusion, my fervent appeal to everyone reading this is to remove the query from your impression, both literally and metaphorically! Instead, phrase impressions using clear unambiguous terms and descriptors, such that both the referring doctor and the patient can clearly comprehend what you are talking about. I would highly encourage individual radiologists, imaging centers, and departments to use the lexicon if possible; the referring physicians just love it and our own thoughts become clearer once we try to commit on a level of certainty for a particular lesion!
– Akshay Baheti, Tata Memorial Hospital
PS: Please feel free to ask questions on the usage of the lexicon or share your thoughts on this in the comments section or on email at caferoentgen@gmail.com

This is another standardized diagnostic certainty scale
https://rad.bwh.harvard.edu/actionable-radiology-reports
Please check it out
LikeLike
Thanks for sharing this Lohith! This looks great, and it’s probably more refined in a sense because it sticks to a smaller set of terms to be used. Coming from my alma mater makes it even more special for me! Akshay
LikeLike