

1. Triple rule out CT – Coronary angiography + aortic angiography + pulmonary angiography:
Done in patients with acute chest pain and suspected cardiovascular cause
Technique:
ECG gating;
100 to 120 ml of contrast at 3.5 to 5 mL/s; 18-20G cannula;
IV ivabredine/ metoprolol (for controlling heart rate)+ nitroglycerine (for vasodilatation) given prior to scanning;
Scan from clavicle to diaphragm;
ROI to trigger the angio placed in ascending aorta
2. Abdominal aortic aneurysm (AAA) is defined as aortic diameter > 1.5 times that of the adjacent aorta. All sizes have to be measured in true axial sections (for an undulating aorta, true axial reconstructions have to be made from the coronal and sagittal reconstructions). Thus, for example, in the AAA below, measurements have to be taken on a 3D workstation by reconstructing in the true axial plane along A, B, C, D, E, and F as shown.

3. Every patient above (or around) 65 years coming for an imaging study (be it USG, CT or MRI) to a radiologist should have screening for AAA included in the report. A single line mentioning the aortic diameters should suffice. Guidelines from the NHS Abdominal Aortic Aneurysm Screening Programme (details on https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/552720/NAAASP_scope_of_practice_document_V2.0_130916.pdf)
- Screening is recommended for everyone 65 years and above
- Ultrasonography is the modality of choice used for screening
- The entire aorta is to be assessed from the level of xiphisternum to the aortic bifurcation
- Maximum anteroposterior diameter (inner to inner diameter) of the aorta perpendicular to the aortic wall should be measured at the lumbar level in both the transverse and longitudinal positions (see figure below for example of correct measurement in longitudinal position).
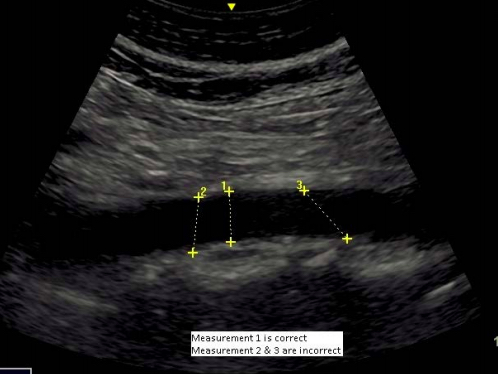
Image obtained from https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/552720/NAAASP_scope_of_practice_document_V2.0_130916.pdf
4. Upon detecting an aortic aneurysm on screening, it is vital to recommend an opinion from a vascular specialist (either interventional radiologist or cardiovascular surgeon). Doing screening of the aorta while performing routine USGs of the abdomen for ANY indication in patients over the age of 65 years is a must. Screening in this manner has shown to decrease mortality from aortic aneurysms by 65%.
5. CT reporting check-list for aneurysms
- Location of the aneurysm and vessels involved
- Probable etiology
- Size –measure outer-to-outer diameter at proximal and distal landing zones, widest diameter of aneurysm from outer wall to outer wall, length of each landing zone, length of aneurysm and combined total length of aneurysm plus both landing zones
- Rate of growth – more than 0.5 cm in 6 months is significant
- Angulation
- Collateral vessels filling the aneurysm sac – if present interventional radiologist can then take appropriate measures to prevent type II endoleak
6. Aneurysm size > 5.5 cm has a 10% risk of rupture and size > 8 cm has a 51% risk of rupture
7. Supra-renal aortic graft is preferred over infra-renal graft as it provides more stability. Infra-renal aortic grafts have a greater tendency for slippage due to smaller landing zone. Supra-renal grafts provide better anchorage.
8. 15 mm of landing zone is traditionally required both proximally and distally to give proper attachment to the stent graft (see figure). A smaller distance may be manageable by newer techniques. A pajama graft (shaped like a pajama) is commonly used to achieve aneurysm occlusion, with the two limbs of the ‘pajama’ going into the two common iliac arteries.
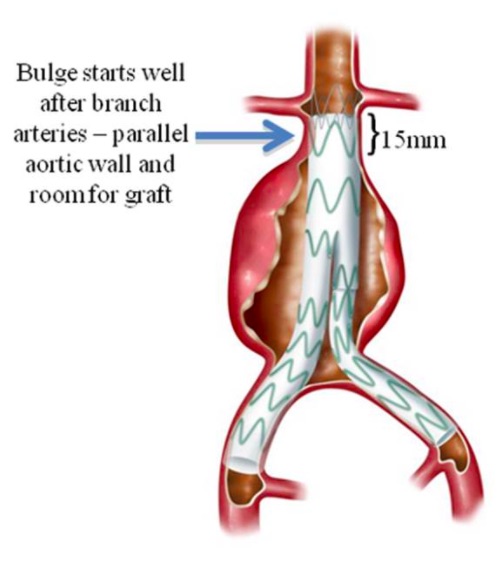
Fig obtained from https://www.iths.org/blog/news/3d-printing-makes-alternative-treatment-for-abdominal-aortic-aneurysms-possible/
9. The diameter of the stent graft selected is approximately 20% larger than the diameter of aorta. Eg. If CT shows an aortic aneurysm with a diameter of 20 mm on the true axial sections, then a graft 20% larger is chosen. Thus the graft deployed in this scenario will be of 24 mm diameter.
10. Whenever performing a CT for aortic aneurysm, the radiologist MUST provide CDs to the patient with images in DICOM format so that the interventional radiologist can use them for appropriate planning with reformatted images along the length of the aorta.
11. First post procedure follow up with CT may be done around 3 months, depending on the protocol of the treating vascular specialist.
12. It is important to obtain delayed phases as well on surveillance CTs for patients after endovascular aortic repair, as active leaks may show up better on the delayed phase.
Reporting checklist:
- Location of aneurysm
- Size of aneurysm
- Rate of growth (compare with previous)
- Presence of endoleak. Collateral vessels filling aneurysm sac if present will be included in this (type II leak)
13. Endoleaks are common complications of aneurysm repair by stent-graft.
They are persistent leaks into the aneurysm sac after stent-graft placement.
Types of endoleaks:
Type 1: Leak into aneurysm sac from either proximal or distal attachment site
Type 2: Leak into aneurysm sac from collateral vessels (most common)
Type 3: Leak from a rupture or tear in the graft material
Type 4: Leak due to endogenous porosity of the graft
Type 5: Endotension (persistent increase in sac diameter without known cause)
Remember;
Type 2 endoleak can be followed up with sequential imaging, as it is a slow leak.
Type 1 and type 3 endoleaks are to be corrected on an emergent basis.
Type 4 endoleak is usually caught by the interventional radiologist immediately after the procedure by doing a catheter angiogram with delayed phase images.
– Ameya Kawthalkar, Senior registrar, Tata Memorial Hospital
– Akshay Baheti, Assistant Professor, Tata Memorial Hospital
Sample template for reporting an aortic aneurysm: (Please note this is just a suggested template and any report you write has to be individualized depending on the patient’s history and findings)
EXAMINATION: CTA of the thoraco-abdominal aorta
CLINICAL INDICATION: …
TECHNIQUE: Dedicated CT angiography of the thoracic and abdominal aorta was performed, covering from the cervicothoracic junction upto the common femoral arteries after intravenous administration of 100 cc of non-ionic contrast.
COMPARISON: (Mention prior CTs available for comparison if it is a follow-up/surveillance scan)
Most recent:
First available (baseline):
FINDINGS:
VASCULAR FINDINGS
(For describing an aneurysm, include: aneurysm saccular/fusiform; extent and/or branch vessel involvement, evidence of atherosclerosis, mural thickening or calcification including branch involvement – see sample description ahead.
For describing dissection, include: level of start and end, branch vessel involvement, branch vessel origin from true or false lumen.)
Measured orthogonal dimensions on current scan:
Aortic annulus: .. mm
Aorta at sinus: .. mm
Sinotubular junction: .. mm
Midascending thoracic aorta: .. mm
Distal arch: .. mm
Proximal descending thoracic aorta (at the level of right pulmonary artery) : .. mm
Distal descending thoracic aorta (at T11-12 interspace) : .. mm
Suprerenal abdominal aorta: .. mm
Infrarenal abdominal aorta (at the level of IMA origin): .. mm
Right common iliac artery: .. mm
Right external iliac artery: .. mm
Left common iliac artery: .. mm
Left external iliac artery: .. mm
(Add a mention on any aberrant vascular anatomy such as accessory renal vessels etc, and on the presence of any atherosclerotic changes; else state that these are absent)
NON VASCULAR FINDINGS:
Chest: …
Abdomen and pelvis: …
IMPRESSION:
For example, here is a sample description of an abdominal aortic aneurysm.
‘There is a large saccular aneurysm at D11 level arising from the anterior wall of the aorta and measuring 8.6 x 8.7 cm in size. There is peripheral thrombus within the aneurysm. The aneurysm extends for a length of 3.7 cm. The celiac artery arises from the caudal aspect of the aneurysm and shows moderate to severe stenosis at the origin with post-stenotic dilatation. The distance between the distal aneurysm and the origin of the SMA is 1 cm.’
For surveillance scan on a patient who has had endograft repair, here is a sample description.
‘There has been an endovascular repair of a thoracic aortic aneurysm.
The endograft extends from just beyond the left subclavian artery origin to the mid descending aorta.
The maximum dimension of the excluded aortic aneurysm is .. mm at the .. level.
The baseline dimensions at same location were .. mm.
There is no evidence of an endoleak, and no signs of stent migration, kinking, or thrombosis.’

Great initiative. Love the notes.
LikeLike
Very nicely and simply explained
LikeLike
Pingback: Abdominal aortic aneurysms sample template for reporting – Cafe Roentgen