

Modalities used for prostate imaging are:
- Abdominal and transrectal Ultrasound
- MRI
- Nuclear Imaging
Ultrasonography has a poorer sensitivity and specificity for detecting and characterizing cancer, and is a better modality for guided biopsy.
Multiparametric MRI prostate is now the standard of care for imaging the prostate and detecting clinically significant cancer (American and European guidelines).
Among the nuclear medicine imaging, PSMA PET/CT far outweighs FDG PET/CT, and is gaining particular importance in detecting biochemical recurrence in a post treatment Ca prostate. It may also sometimes be an adjunct to an MRI for assuring better localization of findings on an MRI in non-surgical candidates and planning for radiation therapy.
We will briefly discuss the recent changes in imaging prostate on an MRI.
ANATOMY OF THE PROSTATE ON MRI
The zonal model of anatomy is based on the ESUR Prostate MRI Guidelines 2012. It employs thirty-nine sectors/regions: Thirty-six for the prostate, two for the seminal vesicles, and one for the external urethral sphincter. Although this may sound daunting, understanding prostate anatomy is as easy (if not easier) than understanding the four lobes of the cerebrum!
The prostate zone on the sagittal sections is divided arbitrarily into three equal parts, namely,
- Base of the gland
- Mid gland
- Apex
These are divided into five unequal zones, well appreciated on a well acquired MRI, namely,
- Peripheral zone
- Transitional zone
- Periurethral zone
- Anterior fibromuscular zone (AFMS)
- Central zone
The bulk of the prostate gland comprises of an outer gland called Peripheral zone which is normally T2 bright and an inner gland called Transitional zone which usually shows heterogenous signal intensity.
Apart from these, a strip of compressed gland around the urethra is called the Periurethral zone; another little larger strip of compressed gland in the anterior midline of the gland is called the Anterior fibromuscular zone (AFMS) and the upper posterior part of the gland at the base through which the ejaculatory ducts course through is called the Central zone.
The anatomical nomenclature of the mid gland and the apex is the same. Whereas, at the base of the prostate, the additional zone seen is the central zone in place of the posteromedial peripheral zone.

Illustration of the zones in the axial section showing the base of the prostate gland (refer to the color code above)

Illustration of the zones in the axial section showing the mid-gland/apex of the prostate gland (refer to the color code above)
MULTIPARAMETRIC MRI PROSTATE (MP-MRIp)
It is the MRI of the Prostate using specific protocol and sequences in order to aid improved detection and staging of prostate cancer.
There is a paradigm shift to detecting clinically significant cancer in treatment naïve population, deciding upon active surveillance when applicable and staging in those detected with significant disease.
Sequences constituting a MP-MRIp
- T2WI (Sagittal; oblique axial and coronal; small and large field of view)
- Diffusion Weighted Imaging with ADC values
- Dynamic post contrast enhancement
- Spectroscopy (This functional imaging tool was more routinely used in the past, but is now losing its relevance due to low sensitivity and lesser incremental diagnostic value. Hence, this is an optional sequence which may be omitted.)
- T1W imaging (large field of view)
FAQs:
1. Which Magnetic strength (Tesla) MRI machine to refer the patient to?
Both 1.5 Tesla or 3 Tesla are good options.
2. Is an MRI endorectal coil mandatory?
No. It is not only not mandatory, but imaging without a coil is sometimes more superior and is surely more cost effective.
3. MRI first or biopsy first?
MRI first whenever feasible.
4. Is an MRI contraindicated in post biopsy scenario?
No. It is always better to defer an MRI after biopsy by about 6 weeks to allow the post-biopsy hemorrhage to resolve. However, if a scan is mandatory for immediate further management, an MRI can be performed (explained below).
5. Post biopsy hemorrhagic areas will hamper a radiologist’s interpretation. Is an MRI still justifiable?
If it is not feasible to wait for 6 weeks, an earlier MRI is still justifiable.
This is because the MRI is performed not simply for diagnosis but mainly for locoregional staging, which is feasible in most cases. The caveat is an inability to diagnose the masked areas, but these areas will be anyways assessed on the already biopsied specimen and hence if malignancy present, the histopathology report will reveal it.
6. What is clinically significant cancer (CSC), biochemical recurrence, Gleason score, and active surveillance?
These are commonly used clinical terms which everyone needs to be aware of.
CSC: The concept of CSC has evolved since many prostate cancers tend to be detected incidentally; the person having such incidentally detected prostate cancer is unlikely to die because of it. While there is no uniform definition of what constitutes CSC, as a concept, it can be regarded as prostate cancer which can cause morbidity or mortality to the patient. Tumors which have high PSA values, bulky disease, and metastatic disease would all constitute CSC, for example. MRI can help detect CSC as very small volume tumors which cannot be seen on the MRI are likely to be insignificant.
Biochemical recurrence: After a patient has been treated for prostate cancer either by surgery or radiation, he will remain under follow-up, usually with PSA levels. Biochemical recurrence of prostate cancer is defined as PSA levels which start rising again after hitting a nadir post treatment. The actual definition is rise by 0.2 ng/mL from the nadir in a patient treated with surgery, and rise by at least 2 ng/mL in a patient treated with radiation. A patient will then be evaluated by imaging (MRI/ PSMA PET) to detect the site of recurrence (whether local or systemic recurrence).
Gleason’s score: This is a pathological grading system used to grade prostate cancer, with higher scores portending worse prognosis. Without going into details, the tumor in the biopsy is graded from 1-5 (1 being well-differentiated and 5 being almost completely undifferentiated). The first part of the score is based on the dominant (most common) pattern of tumor in the specimen and the second half represents the highest grade in the tumor. Thus, unlike conventional mathematics, when it comes to a Gleason’s score, 4+3 is not equal to 3+4. Patients with Gleason’s 4+3 tumors tend to do worse than patients with Gleason’s 3+4 tumors. Generally, overall Gleason’s score upto 6 is low-risk, while scores of 7 or more tend to have higher risk.
Active surveillance: This is a recent concept, but is now an accepted strategy to manage prostate cancer. Under this strategy, patients who have been detected with prostate cancer on biopsy but are deemed to have small non-aggressive tumors need not receive treatment with surgery or radiation. They can instead undergo close regular monitoring to ensure that the disease remains indolent and is not growing.
7. Is a MP-MRI prostate needed for establishing diagnosis of prostate cancer by picking subtle lesions?
No, it is not aimed at detecting only clinically significant prostate cancer. A 12-core prostate biopsy will detect prostate with higher sensitivity, but will however detect many patients with ‘incidental’ cancers of no import, with Gleason’s score of 6. These are likely to be too small to be caught on prostate MRI (ironically our lack of sensitivity is good for the patient in this case!). The utility of MRI is in detecting larger radiologically visible tumors which can harm the patient. It is also used to monitor patients on active surveillance.
8. Are the sequences for PIRADS assessment category same as that of MP-MRIp ?
No, these are a subset of the MP-MRIp. The sequences needed to assess PIRADS category are as follows :
- Small FOV DWI
- Small FOV T2W
- Dynamic post contrast for problem solving
PI-RADS (Prostate Imaging – Reporting And Data Systems)
Current version : Version 2, in application since 2015.
Objective for introducing PIRADS : Improve outcome for patients
Purpose : Improve acquisition, detection, localization, characterization and risk stratification in suspected cancer in treatment naïve prostate gland.
Aims of introducing PIRADS:
- Establish technical parameters
- Standardize terminology and reports
- Facilitate targeted biopsy
- Develop assessment categories to aid in management
- Enable data collection and outcome monitoring.
- Educate radiologists to reduce variability.
- Enhance interdisciplinary communications.
PI-RADS assessment Categories :
These are based purely on MP-MRIp findings.
- PIRADS 1 – Very low (clinically significant cancer is highly unlikely to be present)
- PIRADS 2 – Low (clinically significant cancer is unlikely to be present)
- PIRADS 3 – Intermediate (the presence of clinically significant cancer is equivocal)
- PIRADS 4 – High (clinically significant cancer is likely to be present)
- PIRADS 5 – Very high (clinically significant cancer is highly likely to be present)
Interpretation of findings on T2, DWI and Dynamic post contrast scan
In the peripheral zone, DWI is the most important sequence and DWI findings trump over T2W findings, while it is vice versa in the transition zone. The thing to note on the dynamic contrast scan is presence or absence of early arterial enhancement. Washout characteristics are unimportant.
| DWI-ADC Score | Findings on DWI-ADC in the PZ and TZ
(ADC below the range of 750 -900 um2/s ) |
| 1 | Normal |
| 2 | Indistinctly hypointense |
| 3 | Mild to moderately hypointense |
| 4 | Markedly hypointense <1.5cm |
| 5 | Markedly hypointense >1.5cm, or with ECE |
| T2W Score | Findings on T2W in the PZ and TZ |
| 1 | Normal (Intermediate) |
| 2 | Circumscribed hypointense, or heterogeneously hypointense encapsulated nodule |
| 3 | Heterogenous SI with obscured margins |
| 4 | Non-circumscribed, homogenous, moderately hypointense <1.5cm |
| 5 | Moderately hypointense >1.5cm, or with ECE |
HOW TO APPROACH A MP-MRIp ?
Step 1 : See the entire gland is normal. Report a PIRADS 1.
Step 2 : In case of abnormal findings, rule out benign pathologies. Report these as PIRADS 2. These include :
a. Benign prostatic hyperplasia (BPH) :
Clue on MP-MRIp : Look at the TZ on the T2W sequence. Well circumscribed, capsulated nodules with heterogenous signal intensity and interspersed cystic changes is the hallmark of BPH. (I often call them as a soap bubble like appearance). If in doubt, correlate the suspicious areas with DWI. If the ADC value is significantly low, then consider the finding as more suspicious.
b. Prostatitis:
Often a cause of false interpretation. It is very common in India due to higher incidence of prostatitis, particularly in diabetic men. It is often associated with very high levels of PSA.
Clue on MP-MRIp : Ill-defined low signal intensity on T2 without corresponding significantly low ADC values. Often seen as streaks and bands.
c. Hemorrhage, Cysts, Calcifications
d. Atrophy and fibrosis
Step 3 : In case the abnormal findings are suspicious :
Part a) Scan PZ on DWI.
All those well-circumscribed nodular or geographic areas with low ADC values should be labeled as suspicious. (Impression is not based on T2, but on DWI/ADC in the PZ)
If area of abnormality is less than 1.5 cm, report as PIRADS 4.
If more than 1.5 cm or with extracapsular extension (ECE), report as PIRADS 5.
If in doubt, take the aid of Dynamic post contrast imaging. If the nodule shows early wash in and wash out, report it as PIRADS 4, if not, then report it as PIRADS 3.
Part b) Scan the TZ on T2 (Remember as T for T)
For any finding which is not like a typical BPH, analyze its T2 morphology. All those not circumscribed, ill-defined areas of low signal intensity on T2 with indistinct margins are to be labeled as suspicious.
If area of abnormality is less than 1.5 cm, report as PIRADS 4.
If more than 1.5 cm or with extracapsular extension (ECE), report as PIRADS 5.
If in doubt, take the aid of DWI. If the nodule shows significant low ADC values, report it as PIRADS 4, if not, then report it as PIRADS 3.
Example of a PIRADS 4 lesion in the Transitional zone
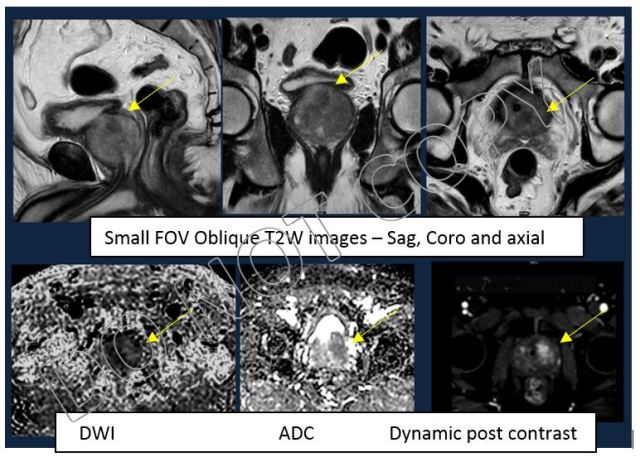 MRI demonstrates a suspicious lesion in the left posterior transition zone at the base of prostate
MRI demonstrates a suspicious lesion in the left posterior transition zone at the base of prostate
Example of a PIRADS 5 lesion in the Transitional zone
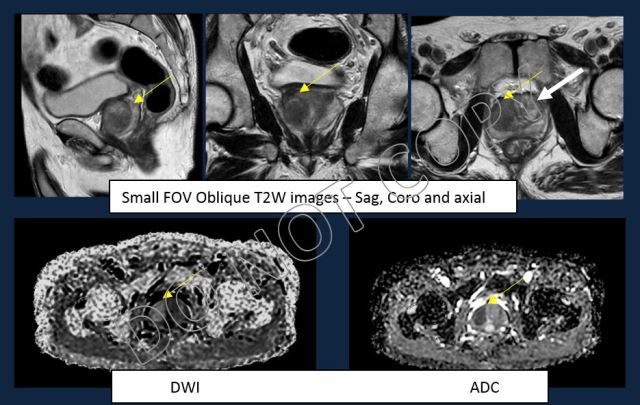
MRI reveals suspicious lesion in the right anterior and posterior transition zone of mid gland of prostate (yellow arrow). The left side of transition zone shows a typical BPH nodule (white arrow).
REPORTING CHECKLIST
- Prostate volume
- Anatomical mapping of the lesion
- Assigning PIRADS ASSESSMENT CATEGORY if treatment naïve. If multiple lesions, the worst score is assigned.
- Lesion size to be written along with Series and Image.
- Staging disease
- ECE
- NV bundle
- Seminal vesicle
- Adenopathy
- Bone metastases
- Incidental findings
Please note that we have covered PIRADS only in brief. For reading more on this topic and for more images, we would recommend a useful article on PIRADS v2 in Radiographics.
– Palak Popat, Assistant Professor, Tata Memorial Hospital
